Australian Medical Network – Open Letter to Atagi & TGA

Fully-referenced grave concerns for vaccines in Australia from Covid Medical Network and Australian pathologists. Despite clear evidence from government-compiled data that the cure is worse than the disease, government officials continue the Safe & Effective Narrative.
Notes from the Open Letter to Atagi, TGA and the Federal Health Department where they are requesting an immediate withdrawal of the experimental gene-based treatments to the general public and especially children.
Covid Medical Network – 8 March 2022 | PDF | Annexures
- I’m going to edit down their letter, keep their references, and add my own references & points (especially to any blog posts I’ve done about what they are bringing up).
- My additions will be bullet points in this colour
- If they’ve mentioned a video, I’ve embedded it.
- If they linked to a url that has moved/changed, I’ve found the archive version and linked to that.
- If you want to read their letter unchanged, please click here.
- Questions to TGA/ATAGI are in this colour
Correspondence from Professor David Healy, Canada
Did you, Professor Skerritt, receive a paper (Evidence Base and Vaccine Policy) and letter from Professor David Healy of McMaster University in Canada?
Annex A – Letter to TGA (Cover) | Annex B – Evidence Base and Vaccine Policy paper (14 pages)
The paper and letter are attached (Annexures A & B) and were sent in mid-December. Prof Healy is an expert in lack of transparency data issues that afflict the conduct of randomised controlled trials, the governance and manipulation of data by trial sponsors, and the integrity of the medical literature, as well as what health regulatory bodies such as the FDA, MHRA, EMA and TGA are privy to or influenced by (02). Such issues are a well-known blight on medical science, that has led to initiatives such as the AllTrials campaign (03).
Prof Healy’s paper raises grave concerns about the conduct of the Pfizer trial upon which vaccine policy in Australia, including to children, is based. It calls upon the TGA to exercise greater vigilance and to pursue Pfizer for the raw data upon which TGA provisional approvals have been granted. His paper notes that without the original raw data to cross reference, manipulation to obscure harms or exaggerate benefits can result in false data being presented in Clinical Study Reports.
According to a FOIA request FOI 2289, the TGA acknowledges to have not obtained individual patient level data (Annexure C and Pfizer Authorized and Data Remains Unseen (04).
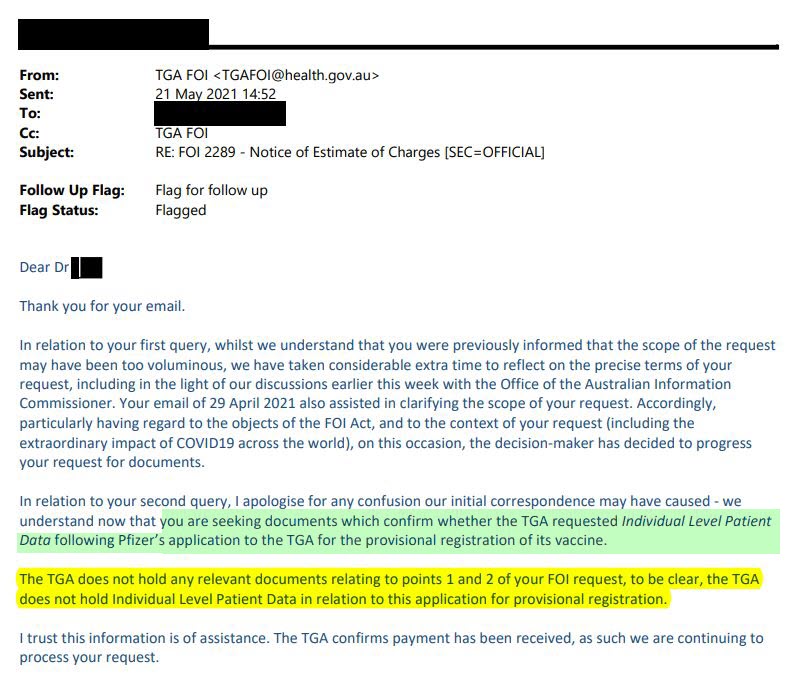

- Australia’s Medicine Regulator has never seen Pfizer Covid Vaccine study data despite deeming it safe for Australians (external link)
- Why Do You Assume Pfizer Are ‘The Good Guys’?
- Pfizer’s Own Trial Data: 1200+ Dead, 46.5% Required Hospitalization & 30% Unrecovered In The First 2 Months & 12 Days Of Rollout
- Corrupt Scientific Medical Research
- Conflict$ of Interest
- Rigged Science & Medicine
- Former Pfizer Staff Speak Out
- 13yo Maddie De Garay [Update 9 Months Later] Permanently Injured From Pfizer Trial
- BMJ editors take on FB Fact-Checkers censorship of the fraudulent Pfizer trials
- [RANT] Pfizer / FDA – Court Released Docs [1st Batch]
- Senator Malcolm Roberts – TGA Fails Duty Of Care To Kids
Previous FOIA requests regarding reproductive toxicology
FOIA requests to the TGA with respect to reproductive toxicology issues have not been adequately responded to, or replied to with heavily redacted documents.
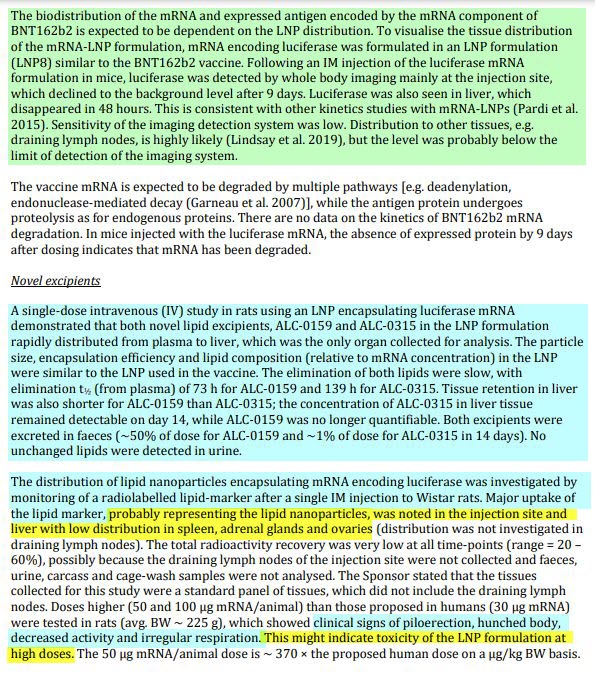
FOI 2389 (Annexure D) noted the serious data of great concern, in Document 6, Submission PM-2020-05461-1-2, that the concentration of labelled mRNA vaccine nanoparticles in rat ovaries is measured at 10x the concentration of nanoparticles in all other organs, with the exception of liver, spleen, adrenals and lymph tissue. But no histopathology of reproductive tissue is noted.
The subsequent FOI 2565 requested “Histopathology/microscopic evaluation of gonads (ovaries/testes) of vaccinated animals in relation to Pfizer and AstraZeneca COVID-19 vaccines”.
This application has been rejected three times, and was rejected finally by the internal reviewers on 27 Sep 2021 (Annexures E & F) – after a refusal on behalf of the requesting party to reduce the suggested scope, and “exclude appendices, annexures and raw data and to withdraw your request for internal review”.


This has become a formal complaint submitted on 25 Oct 2021 (Annexure G).
Withholding reports of ovarian and testicular effects of investigational (provisionally registered), novel, population vaccines is of particular concern in the context of vaccine mandates being imposed upon men and women of reproductive age in various occupational sectors, and now on children and teens with their reproductive years ahead of them.
FOI 3093 is remarkable for its redaction content (Annexures H & I). Report No. 38166, page 60, section 4 Results, section 4.1 Local Tolerance is completely redacted, as is the majority of the following 23 pages. Some concerns regarding uterine swelling and collections of clear fluid in uteri do not appear to have been analyzed any further. Again, there is no histopathology on ovaries to be viewed.

In the information disclosed to date, it appears that the fertility studies have not reached the standards of Developmental and Reproductive Toxicity (DART) studies guided by the European Medicines Agency or the FDA’s Guidance for vaccine development. Gonad histology is not present in the information that the TGA has supplied, despite the repeated requests.
As health care clinicians, we have the responsibility to gather Informed Consent from our patients who justifiably request this information, but we are hindered by AHPRA restrictions from discussing gene-based vaccine potential adverse effects, and the vital information for true Informed Consent is being censored by the TGA.
- TGA – FOI 3093 (External Link)
- The AHPRA Inquisition Against Australian Health Professionals (External Link)
- “Experts” Silenced By Policy
- C-19 Vaccines [Videos] Doctors & Nurses
- Covid Truth With Dr Judy Wilyman
- Aussie Health Workers On Jab Policies
- An Australian Engineer Speaks Out – The Many Mysteries Of Covid
- Laws Against C19 Mandate [Australia] Barrister Raymond Broomhall
- Senator Pauline Hanson Speech – on early treatments banned, vaccine long-term effects unknown – TGA adverse reactions – AHPRA gagged doctors, media censorship, clinical trials, blocking Australian-made vaccines and more.
- COVID Conflict$ Of Interest Australia [Video]
- Verifiable References For Aussies
Recent FOI request regarding molecular genetics data
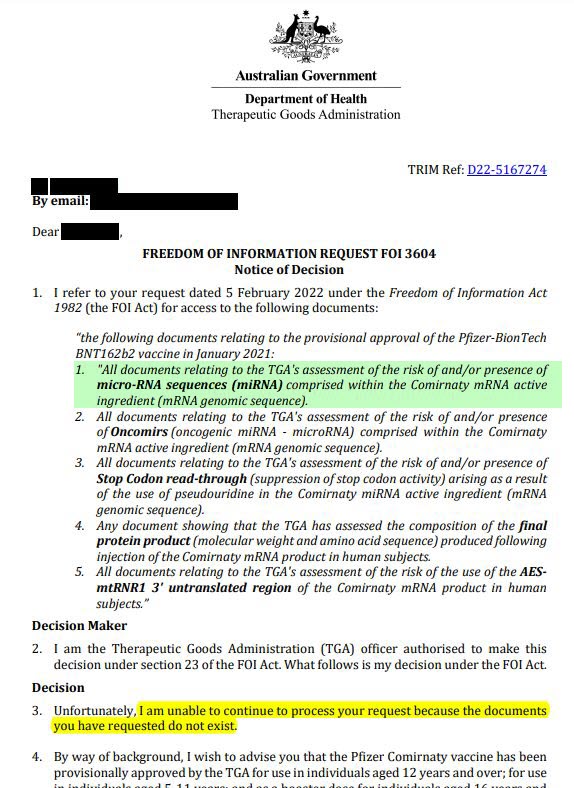
On 18 February 2022, Dr Lisa Kerr of the TGA kindly replied promptly to a FOI request dated 5 February 2022. Dr Kerr’s correspondence is attached (Annexure J) and the lack of requested documents possessed by the TGA is highlighted.

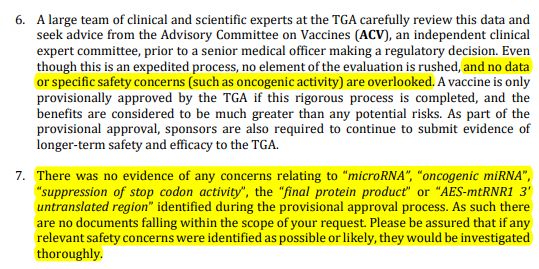


With reference to Items 1 – 5 appearing at Section 1 on page 1 of the correspondence from Dr Kerr, we note the following concerns arising from the failure on the part of the TGA to independently investigate or require the sponsor to fully report its findings, namely:
Item 1
The failure of the TGA to independently investigate, which was further compounded by the failure to require complete sponsor findings in respect of micro-RNA sequences (miRNA) comprised within the Comirnaty mRNA active ingredient (mRNA genomic sequence),
means the TGA never had before it critical information required for a full and proper assessment of Safety for the purpose of evaluating whether to grant Provisional Approval, nor has the Australian community been provided that same critical information for enabling fully Informed Consent to occur, which legal right has therefore been denied the Australian community, on the following issues known by the TGA to involve significant and serious short-, medium-, and long-term safety risks in respect of miRNA, namely:
The Pfizer vaccine sequence is known to contain a number of pathogenic micro-RNA sequences as documented by Fujii (Fujii 2021). (05) These sequences include miRNAs involved in oncogenesis via the WNT-signalling pathway, with unknown long-term effects but likely to involve gynaecological cancers. Additional pathways affected by the encoded microRNAs include inflammatory and pain pathways, again with unknown short- and long-term effects.

Of most concern is the known and documented role that micro-RNAs play in tumour suppression and activation (Ali Syeda 2020), neither action of which can be predicted without experimental evidence. (06)
Thus, there are significant and unknown risks of the miRNAs contained in the vaccine in conferring oncogenic risk either immediately or in the future.
- Quantum microRNA Assessment of COVID-19 RNA Vaccine: Hidden Potency of BNT162b2 SASR-CoV-2 Spike RNA as MicroRNA Vaccine (external link)
- Regulatory Mechanism of MicroRNA Expression in Cancer (external link)
- Sudden Surge In Cancer Within Weeks Of C19 Jabs?
- Spike Genes Have Patented DNA Sequences. This Is Dangerous. (paper review)
- [Legal] Dr David Martin – Paper Trail As Far Back As 1999 Leads To Current Pandemic
- MRNA Vaccines Cause Immune Suppression (Paper – Jan 2022)
Item 2
The failure by the TGA to independently investigate, which was further compounded by the failure to require complete sponsor findings in respect of Oncomirs (oncogenic miRNA – microRNA) in the Comirnaty mRNA active ingredient (mRNA genomic sequence),
means the TGA never had before it critical information required for a full and proper assessment of Safety for the purpose of evaluating whether to grant Provisional Approval, nor has the Australian community been provided that same critical information for enabling fully Informed Consent to occur, which legal right has therefore been denied the Australian community, on the following issues known by the TGA to involve significant and serious short-, medium-, and long-term safety risks in respect of Oncomirs (oncogenic miRNA – microRNA), namely:

As outlined in item 1, microRNAs can have tumour suppressor and tumour activating functions. Tumour activating miRNAs are designated oncomirs. This is a rapidly evolving and new field of genomic medicine about which little is known and therefore the dangers of introducing a new pro-drug that can influence cancer causing pathways are significant. (07)
Item 3
The failure by the TGA to independently investigate, which was further compounded by the failure to require complete sponsor findings in respect of Stop Codon readthrough (suppression of stop codon activity) arising as a result of the use of pseudouridine in the Comirnaty miRNA active ingredient (mRNA genomic sequence),
means the TGA never had before it critical information required for a full and proper assessment of Safety for the purpose of evaluating whether to grant Provisional Approval, nor has the Australian community been provided that same critical information for enabling fully Informed Consent to occur, which legal right has therefore been denied the Australian community, on the following issues known by the TGA to involve significant and serious short-, medium-, and long-term safety risks in respect of Stop Codon read-through, namely:
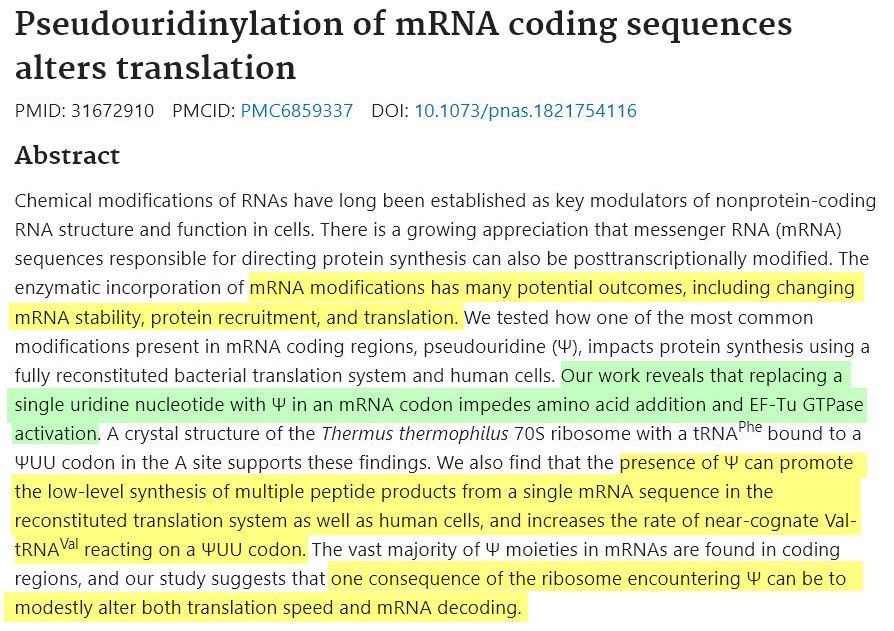
The use of pseudouridine in mRNA vaccines was developed as a very recent concept and its long-term effects are unknown. It has however been known for 10 years that the use of pseudo-U causes the stop codons (required to stop adding amino acids to a protein chain) to misfunction, thereby elongating the protein chain and risking translation of the next segment (the 3’UTR) (Karijolich 2011). The effects of this are unknown and cannot be known without specific experiments to address them. (08)


Furthermore, the use of pseudo-U has major and unknown impacts on microRNA pathways and their concomitant cancer and other pathogenic risks and is a novel field of genomics about which very little is currently known (Lockhart 2019). (09)
Item 4
The failure by the TGA to independently investigate, which was further compounded by the failure to require complete sponsor findings in respect of the composition of the final protein product (molecular weight and amino acid sequence) produced following injection of the Comirnaty mRNA product in human subjects, (Smith 2021) (10)
means the TGA never had before it critical information required for a full and proper assessment of Safety for the purpose of evaluating whether to grant Provisional Approval, nor has the Australian community been provided that same critical information for enabling fully Informed Consent to occur, which legal right has therefore been denied the Australian community, on the following issues known by the TGA to involve significant and serious short-, medium-, and long-term safety risks in respect of the final protein product (molecular weight and amino acid sequence), namely:

It has been known for a number of years that the use of pseudouridine in mRNA can produce final protein products that are not as intended (Eyler 2019). (11)
In addition, the use of artificial 5’ and 3’ untranslated regions and other modifications can produce a final protein product that is not only inconsistent but different in length, shape and function than that which was intended or predicted. The consequences of such changes are unknown but require investigation over long periods of time, including clinical observations of participants of studies for 5-10 years. Failure to create known protein products in a robust and controlled manner can lead to unknown clinical effects including those relating to prion disease which may take many years to manifest (Moreno-Gonzalez 2011). (12)
Item 5
The failure by the TGA to independently investigate, which was further compounded by the failure to require complete sponsor findings in respect of the risk of the use of the AES-mtRNR1 3′ untranslated region of the Comirnaty mRNA product in human subjects,
means the TGA never had before it critical information required for a full and proper assessment of Safety for the purpose of evaluating whether to grant Provisional Approval, nor has the Australian community been provided that same critical information for enabling fully Informed Consent to occur, which legal right has therefore been denied the Australian community, on the following issues known by the TGA to involve significant and serious short-, medium-, and long-term safety risks in respect of the use of the AES-mtRNR1 3′ untranslated region of the Comirnaty mRNA product in human subjects, namely:
mRNA vaccines comprise a genomic sequence of interest (in this case, the SARSCoV-2 spike gene) bounded by untranslated regions (UTR) (5’ preceding and 3’ following) which can be modified to act as biological adjuvants to increase or modify protein production. In the case of the Pfizer vaccine the 3’ UTR (comprising human genomic sequences for AES-mtRNR1) was first developed in around 2018 and the first published use in any animal was in 2019 (Orlandini von Niessen 2019). (13) There were no human studies subsequent to this publication and prior to the combined phase 1-2-3 study the results of which were provided to the TGA for approval. There are therefore no long-term safety studies for this 3’UTR (biological adjuvant).
The Pfizer 3’UTR comprises sequences of human RNA from AES (a tumour suppressor gene) and mtRNR1 (human mitochondrial RNA). Because the intention of any vaccine is to produce immunity against the introduced foreign entity the use of these fragments raises the possibility that immunity may be formed either against the RNA itself (which is 100% homologous to human RNA) or to any peptide products that might be formed due to stop codon read through (see items 3, 4 above). Should this happen the possibility of lupus-related autoimmunity or any other autoimmunity against mitochondrial-dense tissue (such as the heart) becomes a potentially catastrophic risk, given the essential role of mitochondria to the function of major organs. The mechanism of autoimmune disease following Covid-19 vaccination is unknown but is well documented and one of many mechanisms maybe due to antimitochondrial antibody formation (Ghielmetti 2021) in the short term. Autoimmunity against AES, which is a tumour suppressor gene, may equally increase the risk of cancers in the long term. (14)
- Improving mRNA-Based Therapeutic Gene Delivery by Expression-Augmenting 3′ UTRs Identified by Cellular Library Screening (external link)
- Acute autoimmune-like hepatitis with atypical anti-mitochondrial antibody after mRNA COVID-19 vaccination: A novel clinical entity? (external link)
- MRNA Vaccines Cause Immune Suppression (Paper – Jan 2022)
- Virologist Luc Montagnier (1932- Feb 2022) Luc Montagnier who died on the 8th of February 2022, confirmed HIV is in the Spike Protein and has been outspoken along with other virologists about not vaccinating during a pandemic and instead focusing on improving your innate immunity because vaccinating during a pandemic would cause mutant variants, among other warnings such as possible brain and neurological disorders. He is a French Virologist of 78 years and was the winner of the Nobel Prize in Medicine in the year 2008 for discovering the HIV virus and was scheduled to take a part in the Grand Jury Proceeding hearing on February 12, 2022. Just a few weeks before his death, he spoke in the Luxembourg parliament against the mandates, calling the injections poison and not vaccines at all.
- Sudden Surge In Cancer Within Weeks Of C19 Jabs?
- Increased Risk Of HIV Adenovirus Type-5 C19 Vaccines
- Prof. Levi – C19 Vax – Increase In Cardiac Arrests & Heart Attacks
- Heart Damage: MRNA Vaccines (Pfizer/Moderna)
Vaccine generated spike proteins entering human cell nucleus
Is the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health aware of a Swedish in vitro study, published in October 2021 that found that a “surprising … abundance” of full length spike proteins coded for by the gene-based vaccines and produced in the cytoplasm, migrated into the cell nucleus? (15) This was not supposed to happen.
The authors state that once inside the cell nucleus, the spike proteins disrupted “DNA damage repair, especially (that) which lies at the core of B and T cell immunity”. They said:
“Our findings provide evidence of the spike protein hijacking the DNA repair mechanisms machinery and adaptive machinery in vitro. We propose a potential mechanism by which spike proteins may impair adaptive immunity by inhibiting DNA damage repair. … Our findings also imply a potential side effect of the full-length spike-based vaccine.”
SARS-CoV-2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro

- Spike Protein Goes To Nucleus And Impairs DNA Repair (study review)
Dr Mikolaj Raszek, geneticist and biochemist, explains, in his regular YouTube vlog (16) that the TGA’s own document regarding Pfizer’s mRNA vaccine, (Nonclinical Evaluation Report PM-2020-05461-1-2, Annexure D) on page 35 includes results from “Study no. R-20-0360: Analysis of expression of antigens from the mRNA constructs encoding S protein”, that shows blue immunofluorescence in the microscopy of transfected cells indicating spike protein within the cell nucleus. (17)
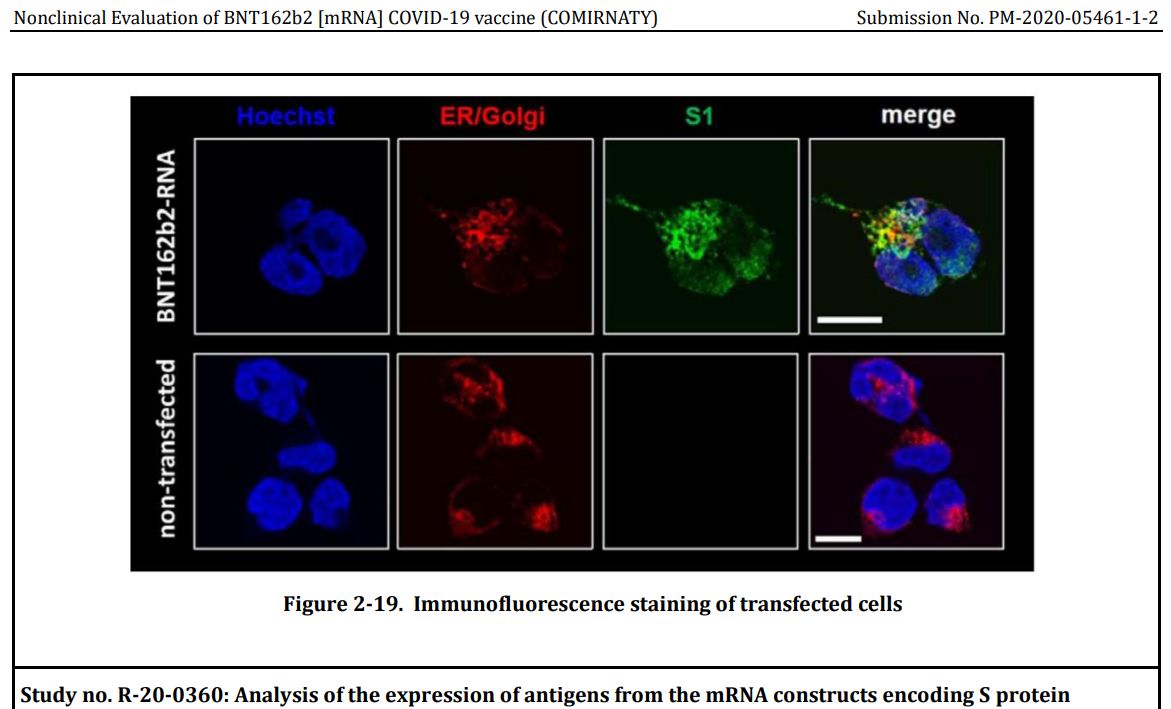
This confirms the Swedish study of Pfizer mRNA vaccine created spike proteins entering the cell nucleus in large numbers.
That spike proteins disrupt DNA repair mechanisms is potentially catastrophic for health. Will the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health be investigating these findings further?
Were you aware that the Nonclinical Evaluation Report on page 35 had this evidence? If so, when was the TGA aware that this finding indicated spike proteins had migrated into the human cell nucleus?
What action will the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health be taking based on this serious finding of risk of DNA repair disruption?
Evidence that mRNA vaccines can be reverse transcribed in human cells
On 23 April 2021 soon after the commencement of the Pfizer and AstraZeneca vaccine rollout, the Australian government department of health on its health.gov.au website reassured clinicians and the public that:
“DNA is stored in the protected centre of our cells – the nucleus. The mRNA is broken down quickly by the body. It never enters the nucleus, and cannot affect or combine with our DNA in any way to change our genetic code.” (18)
However, a Swedish research article by Aldén et al., published 25 February 2022 in Current Issues in Molecular Biology, found evidence that the mRNA sequences from the Pfizer vaccine responsible for coding for the spike protein, are in fact reverse-transcribed into DNA within a human cell line.


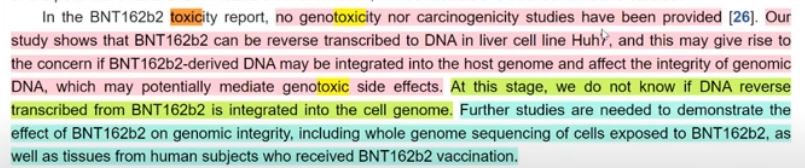
Given that the authors demonstrated a robust response with a factor known to affect the reorganisation of genomic material, this suggested a very real possibility that the RNA sequence from the vaccine may be incorporated into the host cell’s genetic material. This has frightening implications for life-long production of spike proteins within human cells and, if integrated into egg and sperm cells – for intergenerational transmission (Annexure K).
The authors note in the abstract: “We also show that BNT162b2 mRNA is reverse transcribed intracellularly into DNA in as fast as 6 h upon BNT162b@ exposure.”
Given this serious finding of the possibility of genetic modification and pollution of the human genome with foreign genetic material making a toxic protein, will the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health investigate this finding? Will you all issue an advisory warning and take action to halt further harm while investigating this finding?
- Study suggests COVID vaccines could potentially modify people’s DNA – LifeSiteNews (19) (external link)
- Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line (20) (external link)
- Pfizer Vaccine Becomes DNA In Human Liver Cells (In-Vitro Swedish Study) (study review)
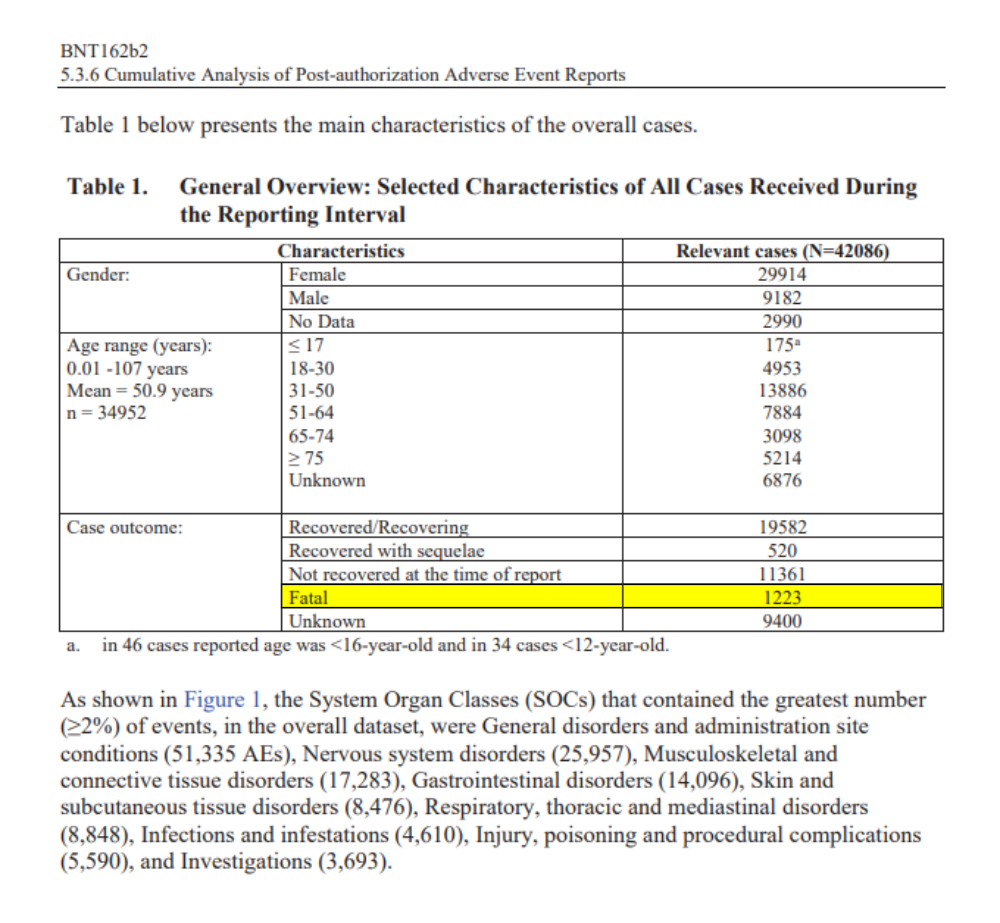
High Pfizer vaccine adverse events data known to the FDA
A FOIA request in the US to the FDA has revealed that the FDA and Pfizer did not make public significant adverse event data from the early rollout of Pfizer to 28 February 2021 (21).


When did the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health become aware of this data?
- Cumulative Analysis of Post-authorization Adverse Event Reports (BNT162B2) 28-FEB-2021 (external link)
- Pfizer’s Own Trial Data: 1200+ Dead, 46.5% Required Hospitalization & 30% Unrecovered In The First 2 Months & 12 Days Of Rollout
- C19 Jabs: More Harm Than Good (500+ Doctors & Scientists)
- 13yo Maddie De Garay [Update 9 Months Later] Permanently Injured From Pfizer Trial
- Pfizer Deaths – Kids (VAERS)
- [RANT] Pfizer / FDA – Court Released Docs [1st Batch]
- Six Months Safety And Efficacy Of Pfizer
Historically unprecedented reports of Adverse Events
It has become abundantly clear to the CMN, that the world has never before witnessed this scale of unprecedented Adverse Event reporting, in respect of only these unique and experimental gene-based vaccines.
It has now become trite to the point of insulting, for any regulator to continue to assert that “correlation is not causation”, and “Adverse Event reporting systems such as the TGA’s DAEN are not reliable”.
The deviation from prior norms for reports on all other vaccines and medications to such Adverse Event databases breaks statistical records.




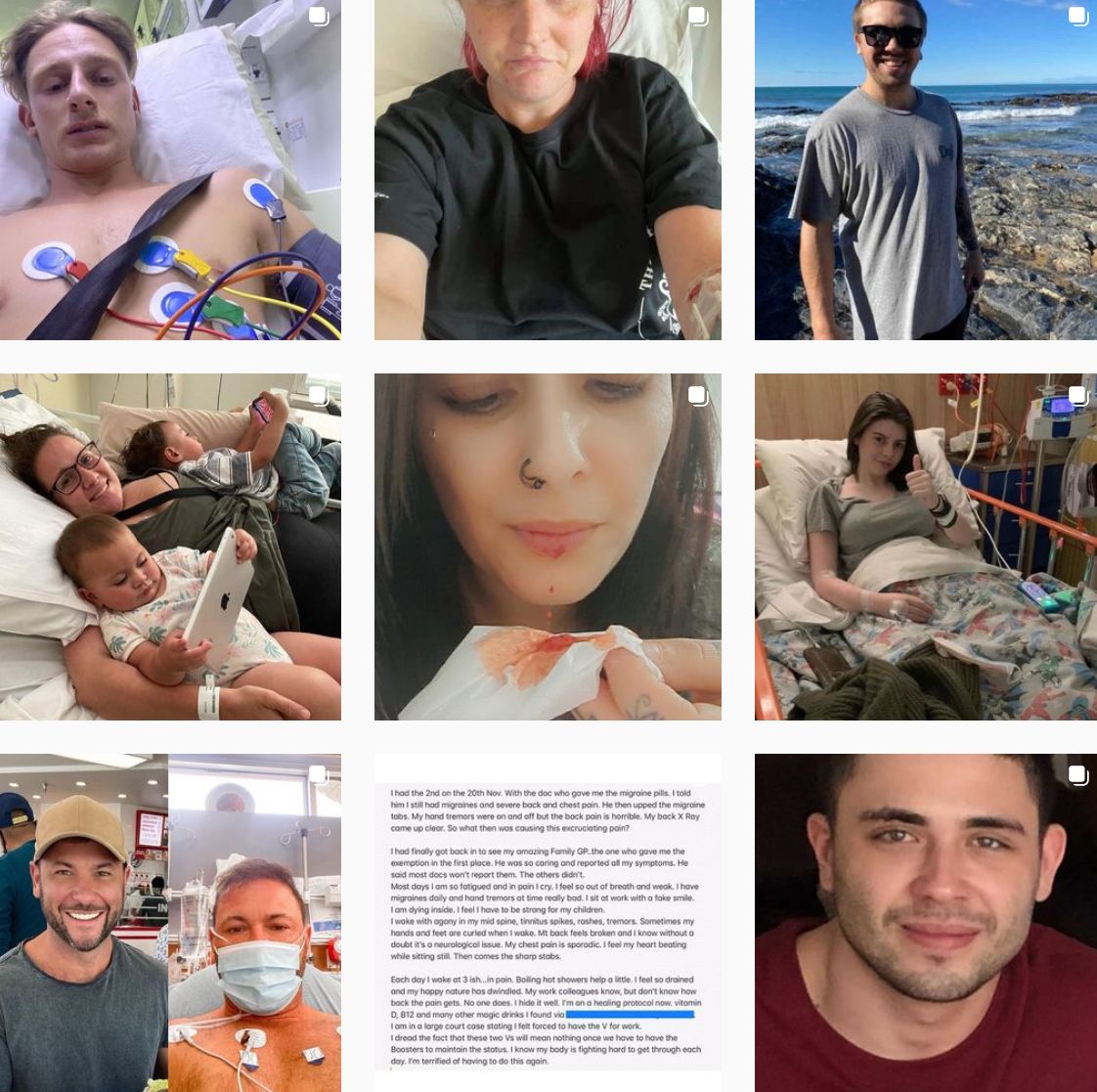










We contend the TGA message of ‘mild and rare events’ associated with the vaccines is not matching the data, nor what is being seen in clinical settings.
Throughout 2021 and continuing unabated into 2022, Australians mostly with the assistance of their physician, are reporting extraordinary numbers of injuries and illnesses suffered and continuing to be suffered from these vaccines, together with recorded deaths from these vaccines, which appear to have likely exceeded deaths from Covid-19 in 2021.
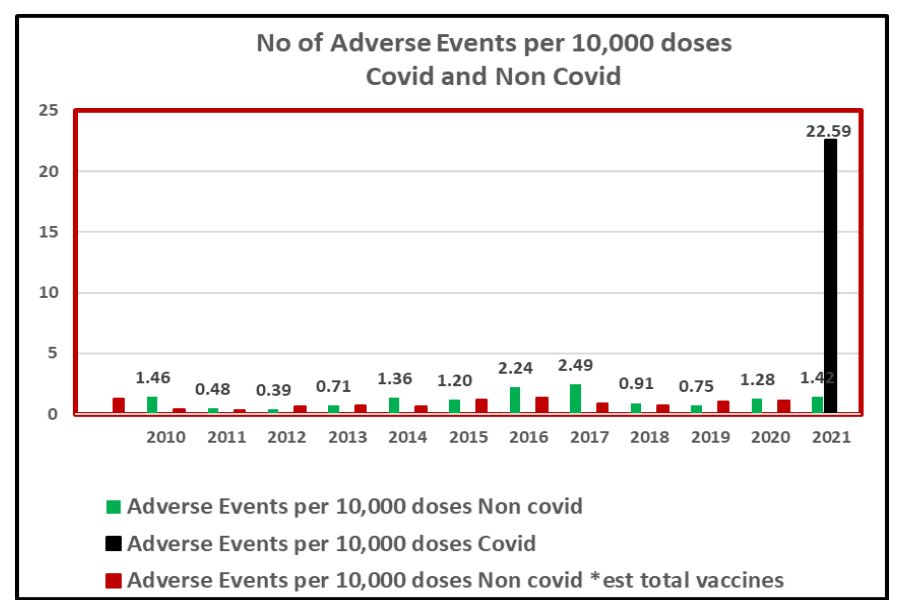
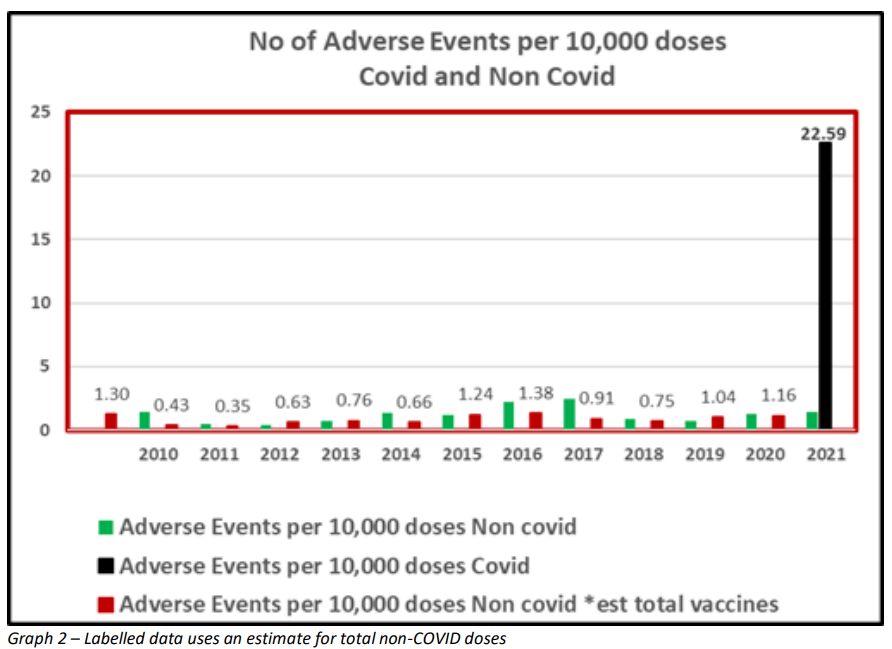
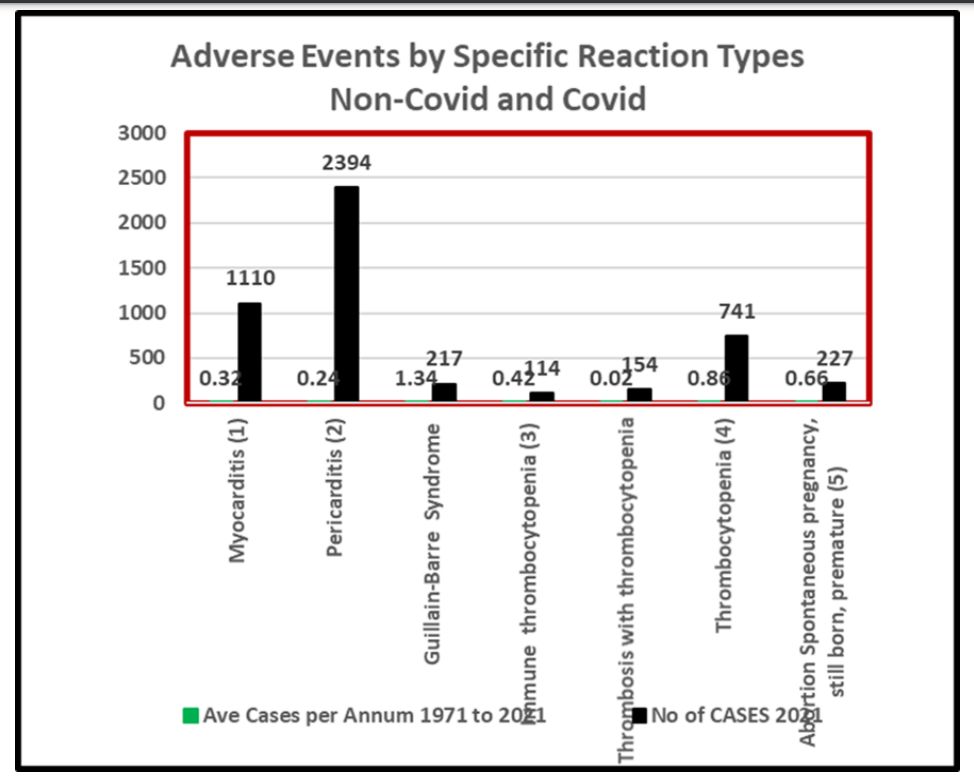
- Annex L A Comparison Of Adverse Events Related Specifically To The Covid Vaccines And Noncovid-19 Vaccines From 1 Jan 1971 To 31 Dec 2021 (PDF – external link)



- Annex M A Comparison Of Adverse Events For Children 5-11 Years Related Specifically To The Comirnaty Vaccine Pfizer And Non-Covid-19 Vaccines From 10 Jan 2022 To 31 Jan 2022 (PDF – External Link)
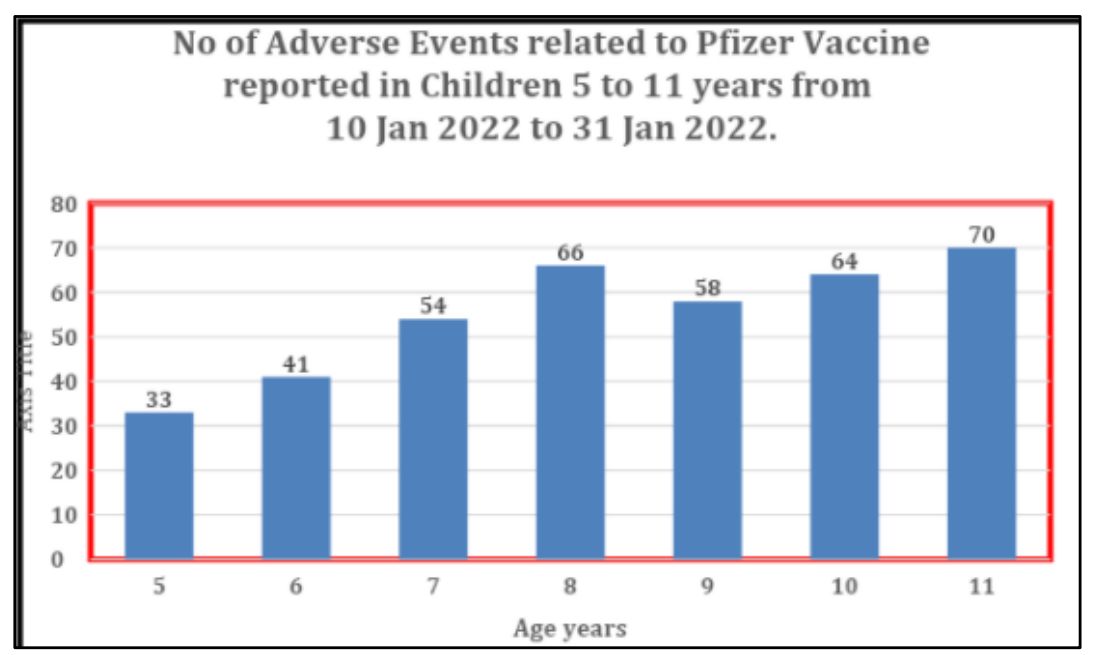
The very troubling lack of transparency or sufficiently detailed explanations for why these adverse event report numbers, as shown in Annexures L & M, should be of paramount concern to a medical community required to administer these vaccines, has not been adequately addressed by the TGA.
Why is the sheer volume of these adverse event reports, to the TGA’s own DAEN database, somehow acceptable to the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, or Delegate of the Secretary or TGA officers and Minister of Health, and when will it be adequately divulged and explained to the Australian medical community?
The medical community, whilst initially split over accepting or not the ‘safe and effective’ assurances regarding experimental gene-based vaccines, is increasingly alarmed as they witness these adverse events. There are now over 109,000 reports of illness, injury, and to date, over 765 deaths possibly causally due to these vaccines. (22) Nothing approaching these data has historically been seen in the DAEN system for other vaccines or drugs. In contrast, Australia averaged just 2.4 deaths per year in respect of traditional protein based vaccines .
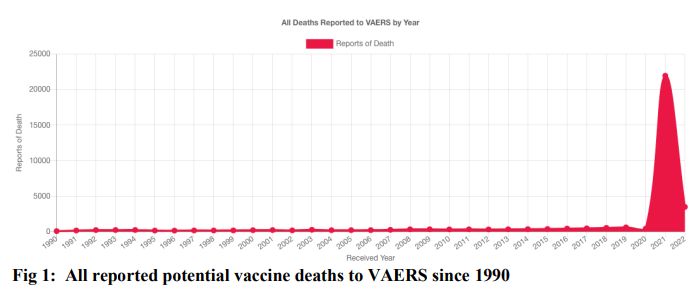
To dismiss these DAEN reports as likely of little consequence, as you, Professor Skerritt, have done in response to Questions on Notice from members of parliament, neglects the fact that they mirror similar patterns of injury reported to the US VAERS, UK Yellow Card, EU Eudravigilance and WHO VigiAccess adverse event databases, and also to the FDA’s own Pfizer adverse event data. The website https://openvaers.com/covid-data (23) collates VAERS data each week. A quick glance shows the contrast in reported mortality for the gene-based Covid-19 vaccines compared to all other vaccines combined since 1990 (fig. 1):
Fig 1: All reported potential vaccine deaths to VAERS since 1990
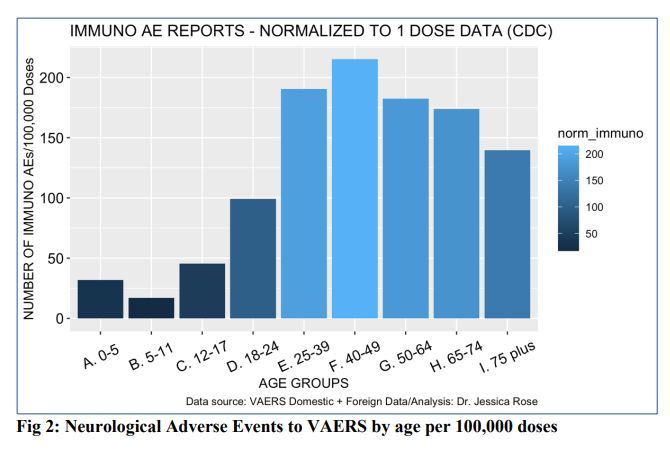
More granular analyses of the VAERS data by virologist, molecular biologist, mathematician and biostatistical data analyst, Dr Jessica Rose, reveals that age stratified data effects younger adults at the highest rate. As younger adults cope with the Covid-19 virus relatively well, this further increases the unfavourable risk/benefit ratio for the gene-based Covid-19 vaccines for those younger than the elderly.
For example (fig. 2), age stratified neurological adverse events normalised to adverse events per 100,000 doses for the 440,175 neurological reports from 319,983 individual cases (24).
Fig 2: Neurological Adverse Events to VAERS by age per 100,000 doses
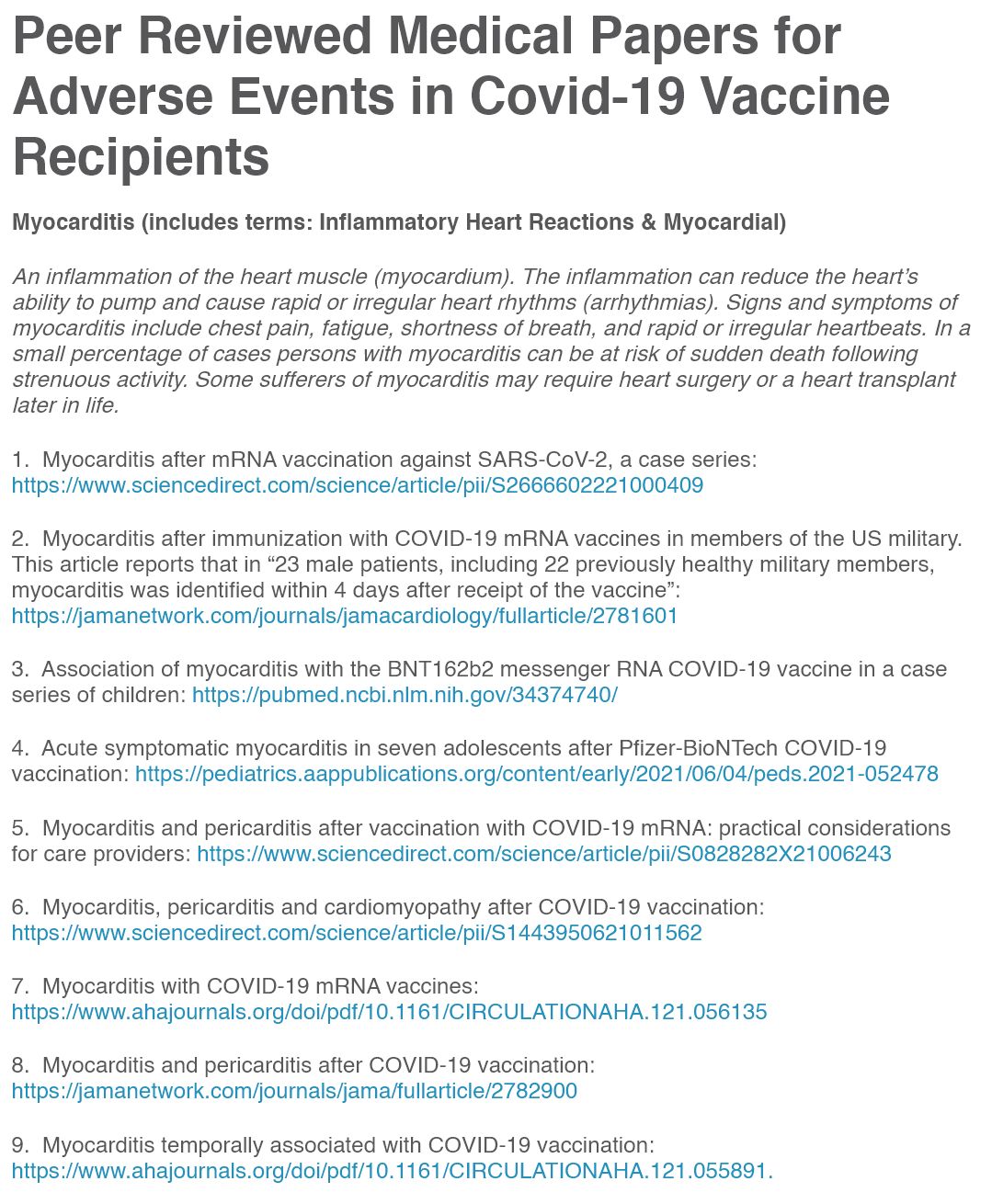
Postulated mechanisms of action of gene-based vaccine injuries are making their way into the published literature and in case reports. Anonymous pathologist, Dr John B., has collated hundreds of relevant papers and case reports (25), and plausible modes of action are increasingly identified.











Of equal import is yet another collection currently holding over 1,000 peer-reviewed papers, speaking to a multitude of adverse events being experienced by Covid-19 vaccine recipients (26).
FOI-3586 is a request to the TGA for data on the deaths reported as possibly related to the Covid-19 vaccines, it is 196 pages long and available online (27). It is almost completely redacted and zero information is available apart from ages of the deceased.
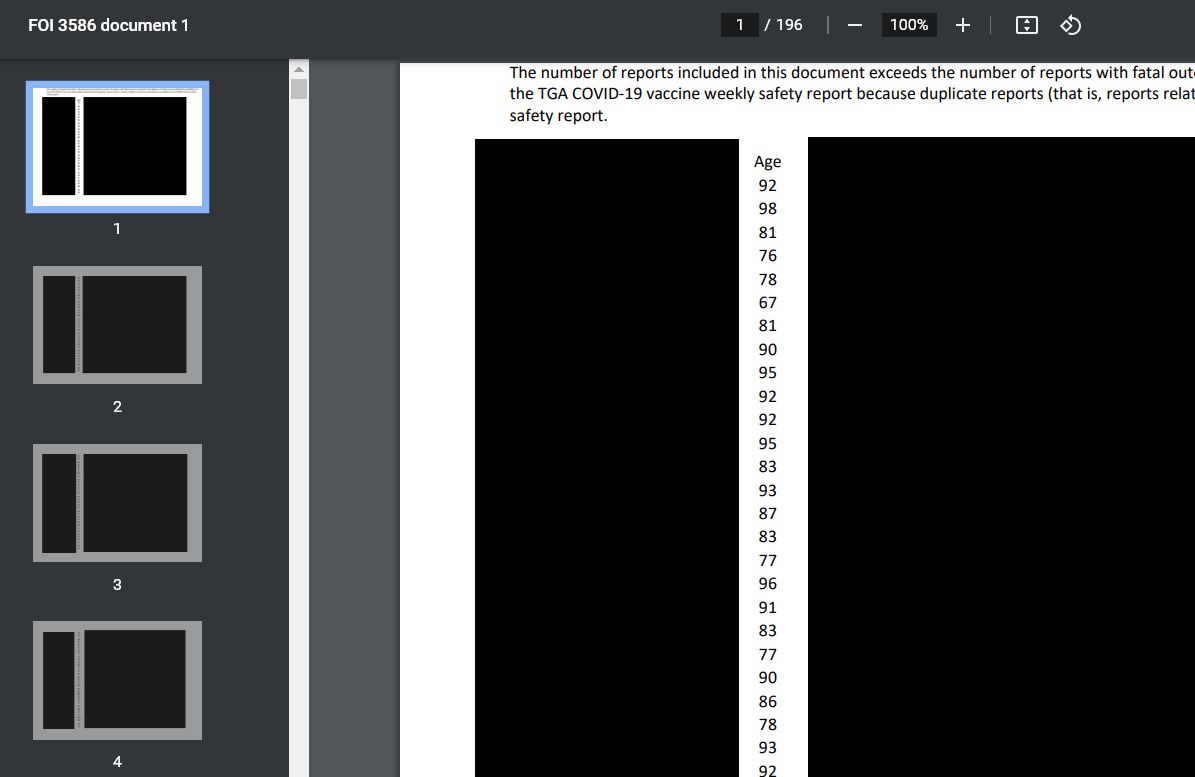

Will the Deputy Secretary, Health Products Regulatory Group or any TGA officer with jurisdiction give reasons for redacting so much data? Will they consider releasing more data, particularly of causes of death, in the public and scientific interest?
FOI-3586 is discussed in more detail below.
The DAEN Under-Reporting Issue
The TGA acknowledges DAEN is affected by under-reporting.

But in the critical context of rolling out an experimental vaccine into the Australian community, continues to refuse to adequately address or accurately quantify the true extent of this data shortcoming, thereby further compromising every individual Australian’s right and ability to give Informed Consent.
Perhaps the Covid Medical Network can assist the TGA and Deputy Secretary in this regard:
In Germany, Adverse Event reporting is compiled by PEI, the Paul-Ehrlrich Institute, much like the United States’ VAERS and the Australian DAEN.
In Annexure N1 & N2 (English machine translation from German) you can view the 21 February 2022 letter from German insurer group BKK ProVita, addressed to Professor Klaus Cichutek of the PEI.
BKK Provita accessed anonymised doctor billing records of over 10Million German citizens, searching for several input codes that showed where patients presented adverse event issues following Covid-19 vaccination. This enabled BKK Provita, using substantial actuarial resources, to conclude the following:



- PEI, who has had the same access to the doctor billing data, has nonetheless been publicly under-reporting Covid-19 vaccine adverse events by a factor of approximately 7.5x; and
- BKK Provita showed that 4-5% of Covid-19 vaccinated people were assessed or received treatment for Covid-19 vaccine side-effects.
The BKK data of its patients has been posted online (28).
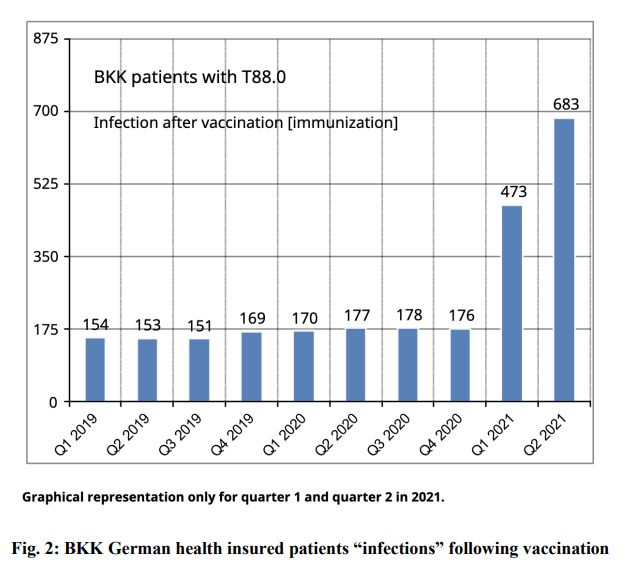
The graphs show a familiar pattern, replicating that of national vaccine injury databases, where adverse reactions (fig. 1) to vaccines have an enormous increase after the rollout of the gene-based Covid-19 vaccines. They also show a marked increase for “infections” (fig. 2), suggesting some immune compromise occurring with this large cohort of German patients.
The advantage of this data is it provides a longitudinal analysis of the health of a defined population, namely the patients of a German health insurance company that keeps detailed data. This is similar to the US DMED data.
Graphs from the BKK data release, translated into English by Dr Jessica Rose (29):
Fig. 1 BKK German health insured patients adverse events following vaccination
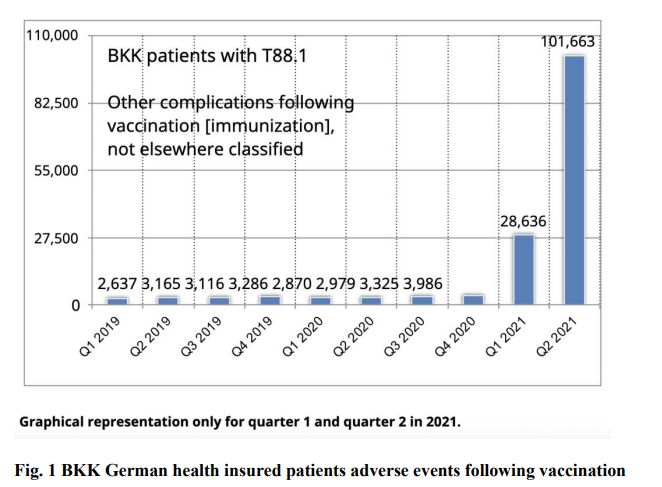
Fig. 2: BKK German health insured patients “infections” following vaccination
In light of the high standards and integrity employed by insurance companies around the world when undertaking statistical analysis of this kind, and the very large number of billing records accessed, together with the complementary evidence coming from other publicly listed insurance companies (see further below), the CMN is confident that the BKK Provita analysis is the best available to date.
However the true state of affairs may be much worse, and possibly with the full knowledge of some individuals. We refer to the TGA’s FOI disclosure log, and particularly FOI document numbered 3586. (31) (32) Document 3586 was returned in answer to the following question:
“The age of deceased for all reported adverse events resulting in death for events reported against any of the TGA approved COVID-19 vaccines.”
Document 3586 contains 197 pages, 169 pages are fully redacted, and 28 pages partially redacted. Of the 28 partially redacted pages, there are 33 reports per page. Those 28 pages show a total of 924 reports of death following Covid-19 vaccination. Therefore the remaining 169 pages contain a further approximately 5,577 cases.
As the question above was quite specific, we see no reason why these additional 169 pages were produced other than to be responsive, and therefore represent reports of deaths following Covid-19 vaccination.
We request the Deputy Secretary and TGA officers that the TGA please un-redact the document, so it can be seen whether the extra pages include reports of suspected or possible Covid-19 gene-based vaccine deaths or not.
So in total document 3586 is prima facie evidence of 5,577 + 924 = 6,501 reports of death following Covid-19 vaccination. Which leaves the CMN confronted with the real possibility that as many as 6,501 Australians have died as a consequence of Covid-19 vaccination.
If we apply the findings of the German pathologists mentioned, taking the mean of 35% applied to 6,501 we arrive at 2,275 deaths causally due to Covid-19 vaccination. However until such time as the Secretary, Deputy Secretary, senior TGA officers, or Government Ministers clarify the true state of affairs, the CMN applies the Precautionary Principle and concludes:
Australians likely to have died as a consequence of receiving a Covid-19 vaccination appear to number somewhere between 2,275 and 6,501.
Again, for Australians who do not have the Covid-19 vulnerabilities of morbid obesity, diabetes and frail elderly status, this likely means that more have died from Covid-19 vaccines than from Covid-19 illness.
This is an abominable state of affairs, bereft of any notion the Hippocratic Oath or the upholding of the Precautionary Principle as alive and well in Australia. Nothing could be further from the truth, in an environment now driven by public health institutions and their officers, extolling politicised and compromised information, at the expense of truth, any respect for Informed Consent, let alone respecting the once sacred and honoured and inviolable doctor-patient relationship.
The CMN invites the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health to clearly and fully correct any and all errors in the above assessment.
- Fully-Vaxxed 9/10 Hospitalizations & 4/5 Deaths (Australia & UK – March 2022)
- More Vaccinated Than Unvaccinated Deaths In Australia (Australia, Scotland, Denmark, Finland, Norway – Jan 2022)
- People Are Still Dying & Hospitalized Even After Being ‘Fully Vaccinated’ (UK, Israel – Oct 2021)
- C19 Victims (Category – View their stories)
- Cannot Prevent Disease Or Transmission, And Worsened Outcomes For Vaccinated Against Delta? (Watch the FDA hearing – Oct 2021)
- Vaccine Boosters? (FDA Hearing – Sept 2021)
- They Are Not Vaccines, People Are Being Killed, & Mandates Are Illegal – Hearing – Prof. Christian Perronne – Jan 2022
- All-Cause Mortality Show Greater Risk Of Fatality After C19 Jabs (UK & USA – Feb 2022)
- [Funeral Industry] Speaking Up About Covid And Boosters (Hear it straight from the people you don’t want to hear it from)
- COVID-19 Spartacus Letter (fully-referenced letter details everything you should know)
- Brazilian President Tells WHO Director “People Are Dying” After C19 Shots, Pleads Not To Recommend To Kids (Nov 2021)
- MRNA C19 Shots: Worse Than Disease? Publication Reviews Possible Future Consequences (goes through everything we know based on the adverse reactions and mechanisms of action from these spike-protein based technologies) May 2021
Excess Mortality in the UK
The United Kingdom led the charge into Covid-19 vaccinations early, therefore their AllCause Mortality data is more robust. The below charts (figs. 1 – 6) were created from data compiled by the UK Office of National Statistics, released 20 December 2021, see:
Deaths involving COVID-19 by vaccination status, England: deaths occurring between 1 January and 31 October 2021. (33) The charts speak for themselves. (34)
Fig. 1: All-Cause Mortality 1 January to 31 October 2021 ages 18–39 years
Rate of death up to 7 times higher in Vaccinated versus Unvaccinated.
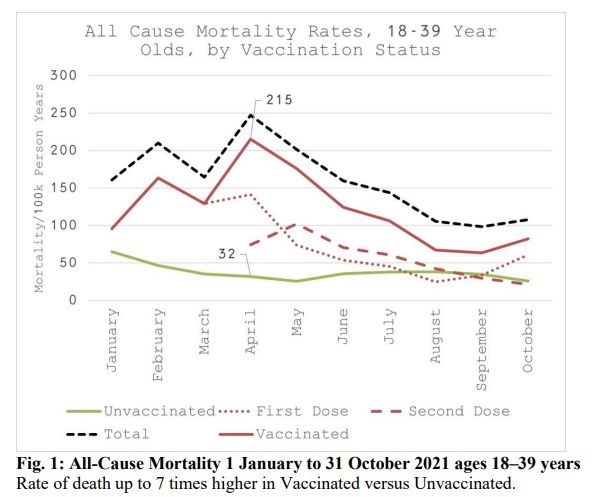
Fig. 2: All-Cause Mortality 1 January to 31 October 2021 ages 40–49 years
Rate of Death up to 3.7 times higher in Vaccinated versus Unvaccinated.
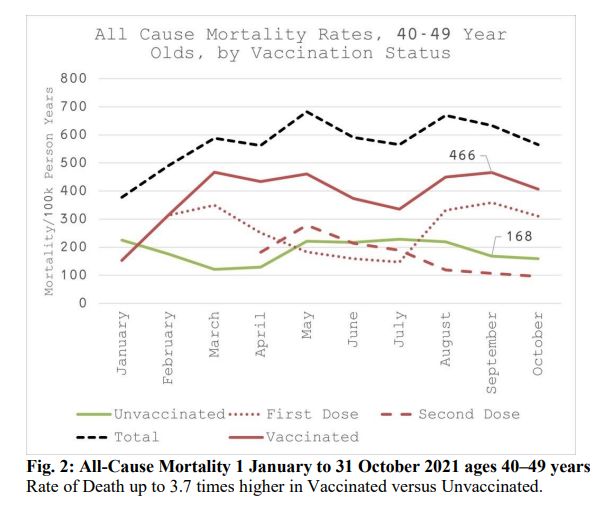
Fig. 3: All-Cause Mortality 1 January to 31 October 2021 ages 50–59 years
Rate of death up to 3 times higher in Vaccinated than Unvaccinated.
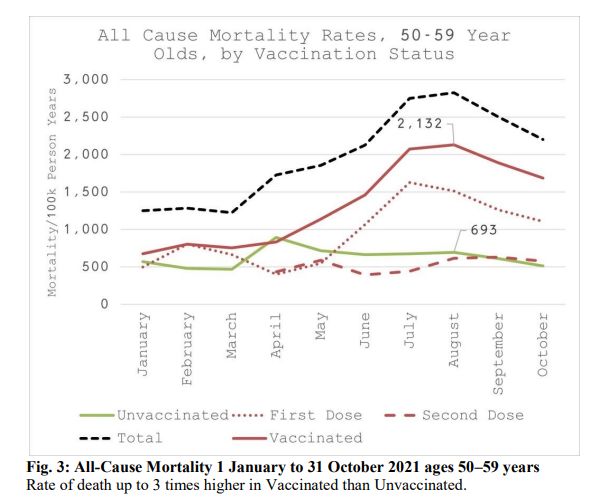
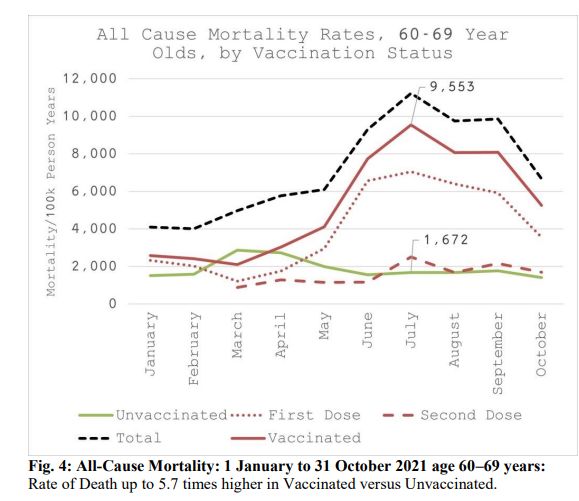
Fig. 4: All-Cause Mortality: 1 January to 31 October 2021 ages 60–69 years:
Rate of Death up to 5.7 times higher in Vaccinated versus Unvaccinated.
5:All-Cause Mortality 1 January to 31 October 2021 ages 70–79 years:
Rate of Death up to 7.8 times higher in Vaccinated versus Unvaccinated.
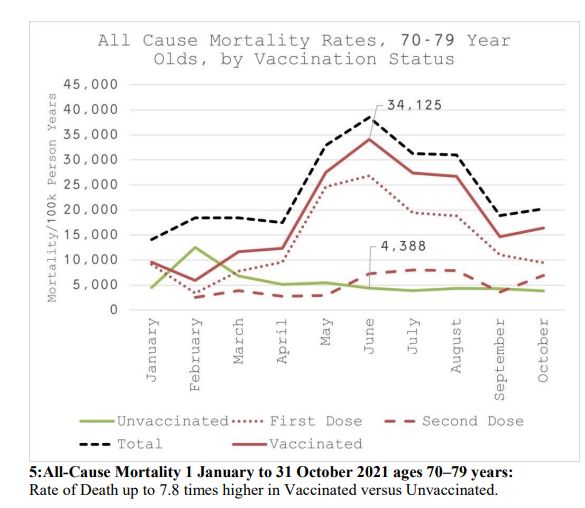
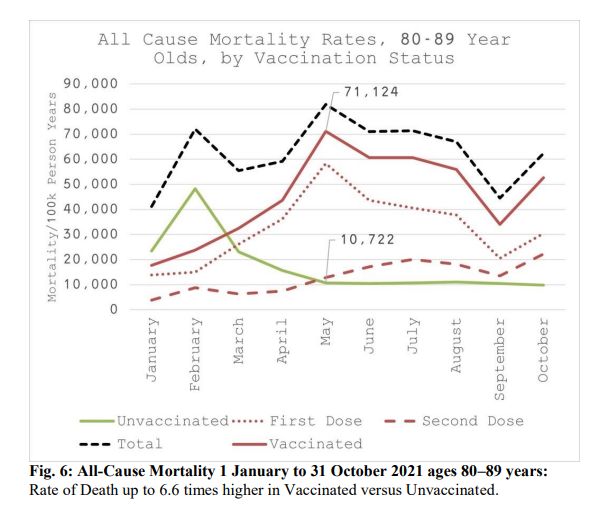
Fig. 6: All-Cause Mortality 1 January to 31 October 2021 ages 80–89 years:
Rate of Death up to 6.6 times higher in Vaccinated versus Unvaccinated.
Excess Mortality in Europe
A brief look at Excess Mortality in Europe (deaths exceeding average All-Cause Mortality occurring in prior years), depicts an equally fatal outcome in 29 European countries throughout 2021 (figs. 7 – 10) (36).
Fig. 7: Excess mortality Europe 2020 (grey), 2021 (blue) ages 15-44.
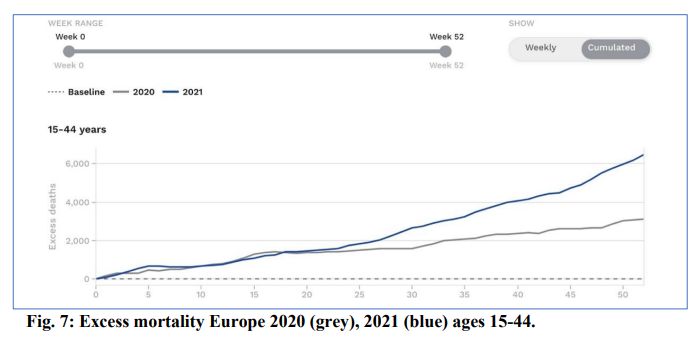
Fig. 8: Excess mortality Europe 2020 (grey), 2021 (blue) ages 45-64.
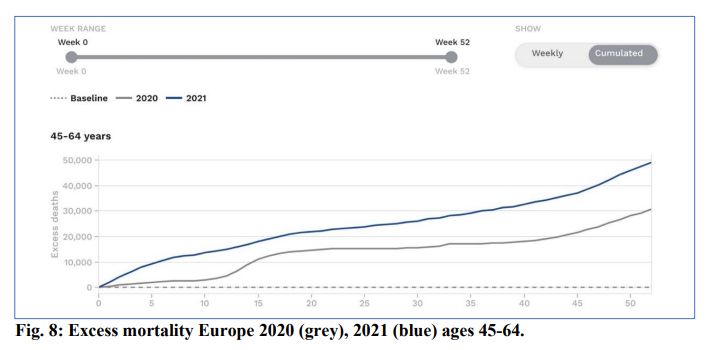
Fig. 9: Excess mortality Europe 2020 (grey), 2021 (blue) ages 65-74.
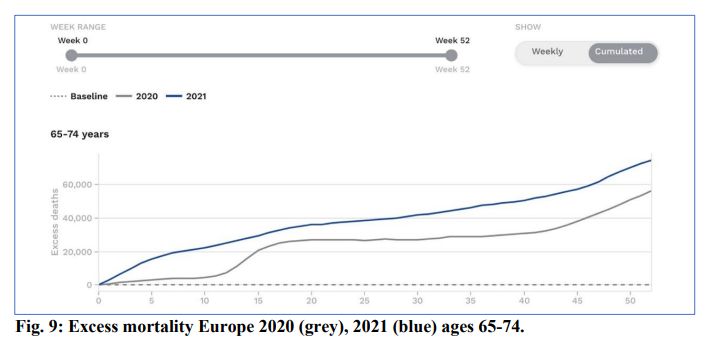
Fig. 10: Excess mortality Europe 2020 (grey), 2021 (blue) ages 75-84.
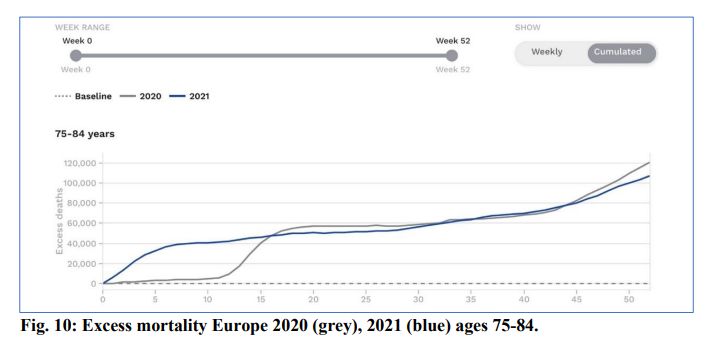
The above charts simply illustrate the rollout of Covid-19 vaccines increased Excess Deaths across Europe, across all age groups, during a year when a less lethal SARS-COV-2 variant of concern, Delta, swept across the globe.
Yet despite this clear evidence from government-compiled data that the cure is worse than the disease, which was available for the internal attention of authorities everywhere, including the TGA, from at least mid-2021, government officials and agencies continued to message relentlessly that these Covid-19 vaccines were, and are, Safe and Effective.
Note: the Excess Deaths across Europe continue unabated into 2022, with the Omicron variant which evades these Covid-19 vaccines, and more severely impacts the Vaccinated. In contrast, the Unvaccinated are showing symptoms akin to mild Influenza (37).
Further, European mortality graphs showing the weekly excess deaths (deviation in mortality from the expected level) for the past years, all ages and by age groups show:
- There were increase waves of deaths in 2020 commensurate with the waves of Covid-19.
- There were greater increases waves of deaths in 2021, compared to 2020, particularly in younger age cohorts, commensurate with the vaccine rollouts, see https://euromomo.eu/graphs-and-maps/: (38).
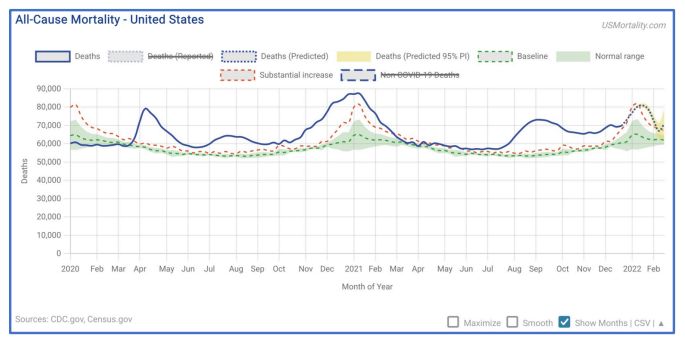
Increase in All-Cause Mortality in the United States 2020 and 2021
As the graph below shows, there was a rise above the normal range for All-Cause Mortality in the USA during the initial Covid-19 wave in March-May 2020, sustained at a lower level through the US summer and then rising with a seasonal winter bulge in November 2020 to February 2021. However, a further large and sustained rise occurred from late July 2021, much higher than the corresponding 2020 summer. By late-July 2021 50% of the US population had received two doses of gene-based vaccines.
Aetiological factors for the US include Covid-19, ‘deaths of despair’ particularly opioid overdoses given impacts on the US economy of lockdowns, but the pattern, commensurate with the VAERS data, the DMED data and US insurance actuarial data, suggests the genebased vaccines are playing a role.
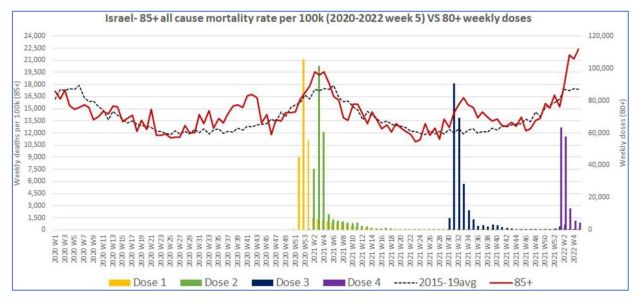
Israeli 85+ years-old age group
Professors Neil and Fenton et al. have noted that official data often labels hospitalisations and deaths as ‘unvaccinated’ when within 2 weeks of a vaccine dose, or sometimes until 2 weeks after the second dose. The rationale for this being that antibodies need to rise for immunity. However, the VAERS and other adverse event reporting system databases show the majority of deaths reported as possibly vaccine-related, occur within the fortnight post vaccine dose.
Israeli data for the elderly show, in late 2020, all deaths were above the previous 5-year trend line, correlating with the Covid-19 pandemic. During periods in 2021 deaths returned to trend line, indicating vaccines probably providing protection from a couple of weeks post second dose and a few weeks post first booster. However, peaks of All-Cause Mortality occurred during and immediately after the initial doses and both booster doses. The present large rise post second booster (fourth dose) is of grave concern, as in the chart below:
Australian All-Cause Mortality 2020 and 2021
2020
In 2020 during the outbreak of SARS-COV-2 there was in fact a decrease in All-Cause Mortality in Australia. Although recent research from Johns Hopkins University in the US indicated lockdowns and Covid-19 restrictions in most nations did very little to stop the spread of the virus (39), Australia’s international and internal border closures and fairly early contact tracing measures provided a more prolonged ‘flattening of the curve’.
The other reason for the Covid-19 pandemic not producing an increase in All-Cause Mortality in Australia in 2020 and only a marginal to modest increase in many other nations, is the fact the lethality of Covid-19 targets mostly the frail elderly. As data from other nations indicated, average age of death from Covid-19 often equates to average lifeexpectancy. That is not the hallmark of a severe all-ages pandemic. This point was made in the Great Barrington Declaration by epidemiologists, public health scientists and thousands of other clinicians and scientists (40).
COVID-19 was only the 38th leading cause of death (898 deaths) in Australia 2020. The median age of death associated with Covid-19 was 86 years, and death occurred in persons already experiencing chronic cardiac conditions, hypertension and/or diabetes prior to death. Indeed, three times (3×) more people died from accidental falls than from Covid-19, see: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/latest-release (41).
2021
In contrast to 2020, and commensurate with the rollout of Covid-19 vaccines in Australia we are confronted with a seriously concerning set of data. During the period 1 January through end of November 2021 Australian health authorities and politicians promoting Covid-19 vaccines need to explain the following:
There were 6,949 deaths (5.4%) more than the 2015-19 average, and
There were 6,264 deaths (4.8%) more than in 2020.
See: https://www.abs.gov.au/statistics/health/causes-death/provisional-mortality-statistics/latest-release (42).
Australian All-Cause Mortality
2015-2019 range blue band, Dec 2020 – Nov 2021
(red line)
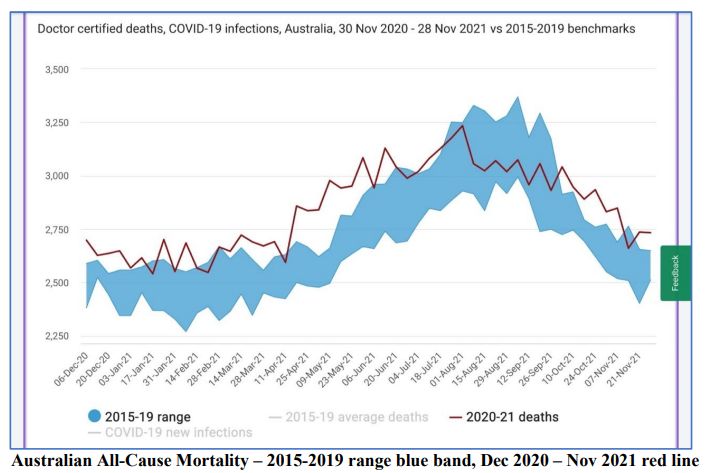
Recall that in 2020 a significantly more virulent and dangerous variant of SARS-COV-2 prevailed. When Covid-19 vaccines became available throughout 2021, the more infectious but less virulent and less lethal Delta, and later, much less virulent and less lethal Omicron variants of SARS-CoV-2 had begun to circulate (see section on Scandinavian and Kaiser Permanente health insurer data on the relatively benign nature of Omicron below).
Yet Australian All-Cause Mortality was 4.8% higher in 2021 than in 2020.
In light of the absence of any major disasters of significance or any other endemic disease of concern throughout 2021, the CMN can point to only one major factor that impacted all Australians throughout 2021, being none other than the concerted campaign undertaken by politicians and government health authorities advocating for the uptake of gene-based Covid19 vaccines, where millions of Australians heeded their call.
To this end the CMN asserts to the Chair of ATAGI, the Secretary of Health, Deputy Secretary of the TGA, and all other noted recipients of this letter, that Australia’s marked increase in All-Cause Mortality in 2021 was most likely causally due to these experimental Covid-19 vaccines.
- [Rant] More Vaccinated Than Unvaccinated Deaths In Australia
- Aussie Nurses, Paramedics, Health Workers Speak Out About COVID-19 Vaccine Injuries
- Fully-Vaxxed 9/10 Hospitalizations & 4/5 Deaths (Australia & UK, Jan-Mar 2022)
- Against Our Will [Australia & New Zealand]
- Verifiable References For Aussies
- Health Insights From The First Year Of COVID-19 In Australia
- Fair Work Commission On COVID-19
- Infection Fatality Rate Of <0.1% For Those Aged Under 70
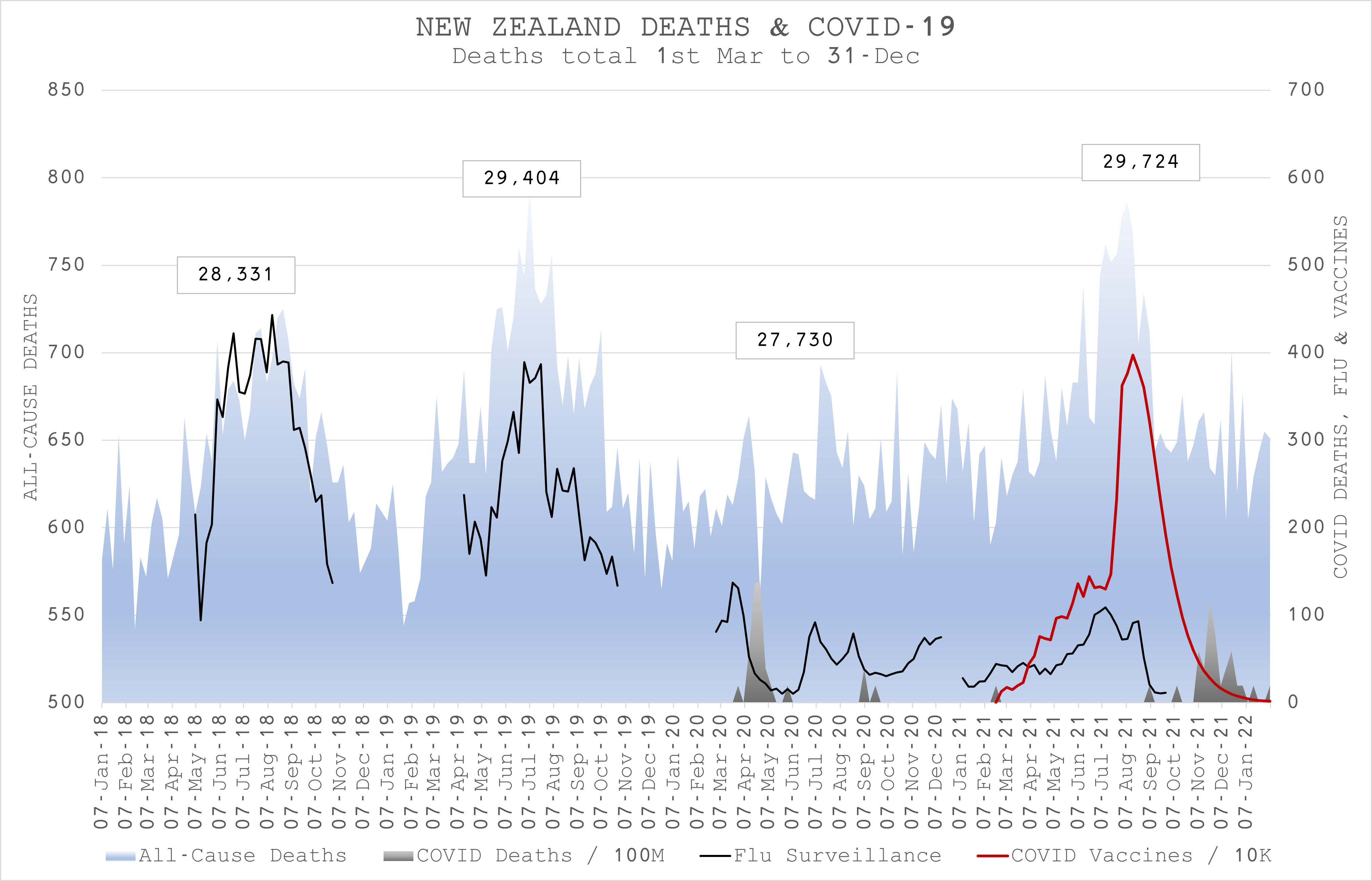
New Zealand All-Cause Mortality correlates with vaccine rollout in 2021
Joel Smalley is an independent researcher who has collaborated with the biostatistical research group from St Marys College, University of London. He has analysed New Zealand All-Cause Mortality in the graph below for years 2018 – 2021.
The death counts correlate highly with influenza seasons in 2018 and 2019 and there was a marked decrease in deaths in New Zealand with collapse in influenza numbers – and few cases of Covid-19 corresponding with New Zealand’s closed borders and lockdowns. However, in 2021, despite similar low rates of influenza and, prior to November almost ‘Zero-Covid’, All-Cause Mortality death rate was highest, correlating temporally with the gene-based Covid-19 vaccine rollout
United States Defence Medical Epidemiology Database (DMED) rates of illness
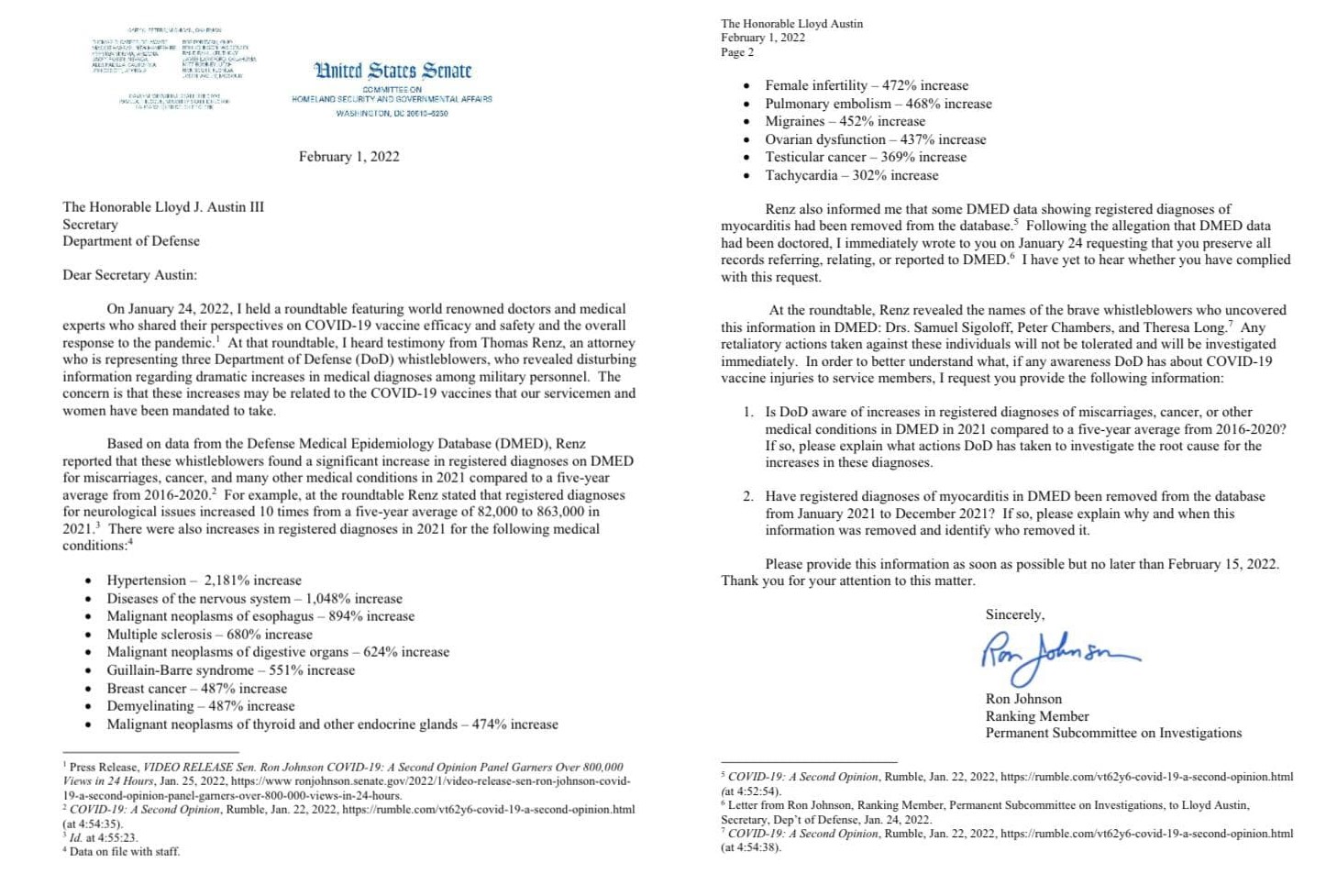
Recent allegations of increased illnesses amongst US military personnel warrant mention because the three named whistleblowers were all military doctors and two had ranks of Lieutenant-Colonel. Attorney Thomas Renz reported to a hearing in Washington DC under the auspices of Senator Ron Johnson (R-WI) that the three military doctors had reviewed the data of the Defence Medical Epidemiology Database (DMED) and compared the rates of diagnoses in 2021 following the gene-based vaccine rollout with the previous 2016-2020 five-year average that included the first year of the pandemic.
Attorney Renz reported that the military doctors, are presenting the data “under penalty of perjury” and found extremely high increases in rates of diagnoses, for example:
- neurological disorders: 1048%;
- breast cancer: 487%;
- disseminated intravascular coagulation: 1,175%;
- pulmonary embolisms: 468%;
- myocardial infarction: 269%;
- spontaneous abortion: 279%;
- congenital malformations for neonates: 156%;
- female infertility: 472%.
The Senator has officially written to the US Secretary of Defense about these alleged findings (44).
The pattern of diagnoses follows that of the official databases and the FOIA released Pfizer-FDA adverse events data. Given that military doctors are supposed to record diagnoses in the DMED, the data might, if confirmed, be a more accurate gauge of the adverse events rates than passive reporting systems such as VAERS and DAEN.
In response, the US Department of Defence has not disputed the high rates of 2021 diagnoses but has argued that the previous five year rates were under-diagnosed by similar rates. That explanation would, as Attorney Renz has argued, undermine and invalidate published epidemiological research based on DMED data, and indicate that the US military has worryingly high rates of ill-health, which frankly stretches credibility and warrants further urgent auditing.
Is the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health aware of these US military whistleblower allegations and of US Senator Ron Johnson’s letter to the US Secretary of Defence? If so, are the Chair of ATAGI, the Secretary of Health, the CMO or the Deputy Secretary of the TGA or senior TGA officers making inquiries as to the veracity of these claims of multi-fold increases in various medical disorders since the mandating of gene-based vaccines to the US military?
German pathologists’ autopsy findings attributed to vaccine injury
Of grave concern are findings in a case series of autopsies and biopsies from people with suspected gene-based vaccine related mortality and morbidity, conducted by a group of experienced German pathologists. In this interview (45) with German virologist Prof Sucharit Bhakdi, experienced pathologist Prof Arne Burkhardt reports findings of lymphocytosis – large unusual infiltrations of lymphocytes into inflamed organs pertaining to the morbidity of the deceased.
The lymphocyte deposits are generally accompanied by infiltrations of gene-based vaccine manufactured spike proteins. He states that these findings have never been seen prior to the spike protein from the gene-based vaccines.
Prof Burkhardt provides histological evidence in the linked video. The findings of spike proteins and lymphocyte infiltrations are primarily in endothelial cells of blood vessels and contribute to clotting and inflammation of arteries. In the meninges and brain tissue these infiltrates contributed to subarachnoid haemorrhage, encephalitis and small vessel inflammation of the brain, In major arteries they contributed to coronary artery occlusion and aortic rupture, while, in the spleen, very large lymphocyte aggregates Prof Burkhardt and colleagues described as “pseudolymphoma” contributed to splenic artery occlusion.
More recently Prof Burkhardt and colleague Prof Walter Lang presented autopsy proof of a person who died 4 months post vaccine, of vaccine manufactured spike proteins as the causative agent in lesions in blood vessels as well as myocarditis (46).
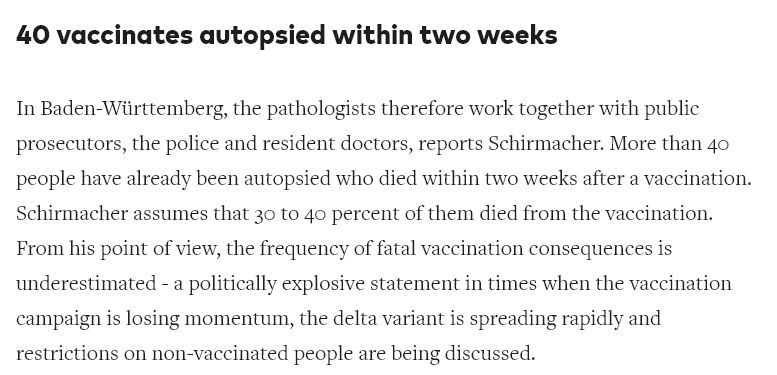
In a separate report, Heidelberg’s chief pathologist, Dr Peter Schirmacher, autopsied 40 patients post-vaccination in a fortnight and estimated 30–40% of them had died because of the vaccine. He received criticism by the authorities but was supported by the German college of pathologists. The story did not make any English news media, (but can be Google translated – Annexure P (47).

Around the globe, despite record numbers of deaths temporally associated with the genebased vaccines reported to the official databases such as DAEN, there have been surprisingly few autopsies. The German pathology groups’ series calls out for more autopsies and research.
Are any of the C Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health aware of these autopsy findings by experienced German pathologists?
Has the Chair of ATAGI, the Secretary of Health, the CMO or the Deputy Secretary of the TGA provided guidance and additional resources and assistance, for a greater number of autopsies for Australians whose deaths are reported to DAEN as possibly related to the Covid-19 gene-based vaccines? If so, please evidence what guidance and additional resources and assistance have been provided to those responsible for conducting autopsies for Australians whose deaths are reported to DAEN as possibly related to the Covid-19 gene-based vaccines, together with the distribution list of recipients.
Further, has the TGA provided guidance to pathologists and pathology groups performing autopsies on those known to have received one or more Covid-19 vaccines, so correct testing is carried out for answering whether causality can be ascribed to a Covid-19 vaccine? If so, please furnish copies of any such guidance, together with distribution list of recipients.
Has the TGA issued any directives or advices to pathologists seeking to answer this question of Covid-19 vaccine causality, by alerting pathology groups to the following papers? If so, please furnish copies of any such directives or advices, together with the distribution list of recipients.
- Postmortem investigation of fatalities following vaccination with COVID-19 vaccines. Int J Legal Med. 2021 Nov;135(6):2335-2345. doi: 10.1007/s00414-021-02706-9. Epub 2021 Sep 30. PMID: 34591186; PMCID: PMC8482743. (48)
- Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings. J Korean Med Sci. 2021 Oct 18;36(40):e286. doi: 10.3346/jkms.2021.36.e286. PMID: 34664804; PMCID: PMC8524235. (49)
- Autopsy Findings and Causality Relationship between Death and COVID-19 Vaccination: A Systematic Review. J Clin Med. 2021 Dec 15;10(24):5876. doi: 10.3390/jcm10245876. PMID: 34945172; PMCID: PMC8709364. (50)
- An Insight into the Role of Postmortem Immunohistochemistry in the Comprehension of the Inflammatory Pathophysiology of COVID-19 Disease and Vaccine-Related Thrombotic Adverse Events: A Narrative Review. Int J Mol Sci. 2021 Nov 6;22(21):12024. doi: 10.3390/ijms222112024. PMID: 34769454; PMCID: PMC8584583. (51)
- Pomara C, Salerno M, Esposito M, Sessa F, Certo F, Tripodo C, Rappa F, Barbagallo GM. Histological and immunohistochemical findings in a fatal case of thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. Pathol Res Pract. 2022 Mar;231:153796. doi: 10.1016/j.prp.2022.153796. Epub 2022 Feb 4. PMID: 35144085. (52)
- Deaths associated with newly launched SARS-CoV-2 vaccination (Comirnaty®). Leg Med (Tokyo). 2021 Jul;51:101895. doi: 10.1016/j.legalmed.2021.101895. Epub 2021 Apr 17. PMID: 33895650; PMCID: PMC8052499. (53)
- COVID-19 Vaccine and Death: Causality Algorithm According to the WHO Eligibility Diagnosis. Diagnostics (Basel). 2021 May 26;11(6):955. doi: 10.3390/diagnostics11060955. PMID: 34073536; PMCID: PMC8229116. (54)
BMJ reporting of Pfizer trial irregularities
These FOIA revelations and adverse event data indicating that all was not right with the Pfizer Covid mRNA vaccine data are supported by testimonies from three conductors of the clinical trial, as described in the British Medical Journal (BMJ) in a 2 November 2021 article titled “Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial” (55). The whistleblowers reported that the clinical trial contractor company, Ventavia, conducting the Pfizer trial: “falsified data, unblinded patients, employed inadequately trained vaccinators, slow to follow up adverse events … mislabelled laboratory specimens, vaccines not stored at proper temperatures … lacked employees to swab all possible Covid cases”.
- BMJ: Unclean Data In Vaccine Trials (Pfizer & FDA Should Be Investigated & Rollout Halted)
- Pfizer’s Own Trial Data: 1200+ Dead, 46.5% Required Hospitalization & 30% Unrecovered In The First 2 Months & 12 Days Of Rollout
- 13yo Maddie De Garay [Update 9 Months Later] Permanently Injured From Pfizer Trial
As BMJ senior editor Professor Peter Doshi notes, thousands of trial participants with flu-like symptoms appear not to have been swab tested for Covid (56). In a recent BMJ editorial, Professor Doshi concludes that Pfizer and other companies cannot be trusted, and that regulators, academic journals, the medical profession and the general public all need access to the full data (57)
Thus, the likelihood that the Pfizer data, upon which the TGA based its provisional authorisation, is skewed towards minimising harms and exaggerating benefits is high. You may of course have information that contradicts this. In the interests of transparency about harms and benefits of a mandated vaccine, we request you please respond to us?
However, as below, the issue is now before the courts in the United States.
Anomalies and impurities seen in vaccine vial samples and blood films
The CMN views reports of anomalies and impurities in vaccine vials, that correlate with similar findings in microscopic examination of live blood films, with consternation and alarm. Such reports are becoming more numerous and replicated from laboratories and practitioners around the world. The issue of metallic foreign substances in the Moderna vaccines made the news from contaminated batches in Japan (81), so quality assurance issues with the vaccines are real.
However, scientists now report what they believe are findings of graphene, as per a brief presentation from the World Council for Health of spectroscopy findings in 1 Pfizer, 2 Moderna and 1 AstraZeneca vials (82).

Annexure U has been authored by Australian pathologists and shows photographs of blood samples and vaccine samples with strange anomalies viewed via an array of microscopy techniques and correlating with similar findings from other researchers and practitioners overseas.
To quote our Australian pathologist colleagues:
“Numerous researchers around the world have also examined the Pfizer, AZ, Moderna or J&J covid vaccines and have reported seeing the same anomalies. Optical Microscopy, BrightField Microscopy, pHase Contrast Microscopy, Dark-Field Microscopy, UV absorbance and Fluorescence Spectroscopy, Raman spectroscopy analysis, Scanning Electron Microscopy, Transmission Electron Microscopy, Energy Dispersive Spectroscopy, X-ray Diffractometer and Nuclear Magnetic Resonance instruments were used to verify the vaccines morphologies and contents. They have reported seeing similar anomalies … Again, the scientific community are shocked by these findings of undisclosed suspicious ingredients in the covid vaccines. We believe, at a bare minimum, this warrants an explanation and further thorough investigation to be able to give the Australian public true informed consent.”
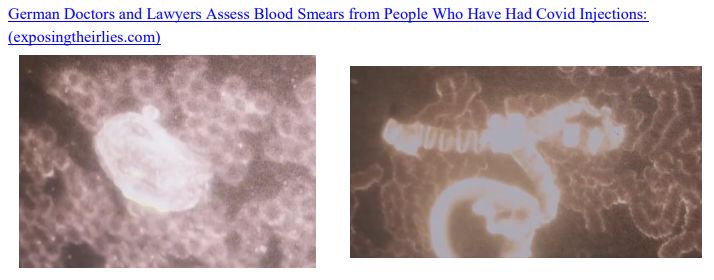
In August 2021 Dr. Bärbel Ghitalla reported live blood analysis on her vaccinated patients. Results showed red blood cells (RBC) ‘stacking’ one upon the other and several unusual objects. The photo on the left at 400x magnification shows these stacked RBS ‘rouleaux’ formations surrounding an unusual large black crystal. The right hand picture at 100X magnification shows significant rouleaux and coiled pieces of something large and long with a metallic sheen. They could easily be seen and did not absorb light as red blood cells do.
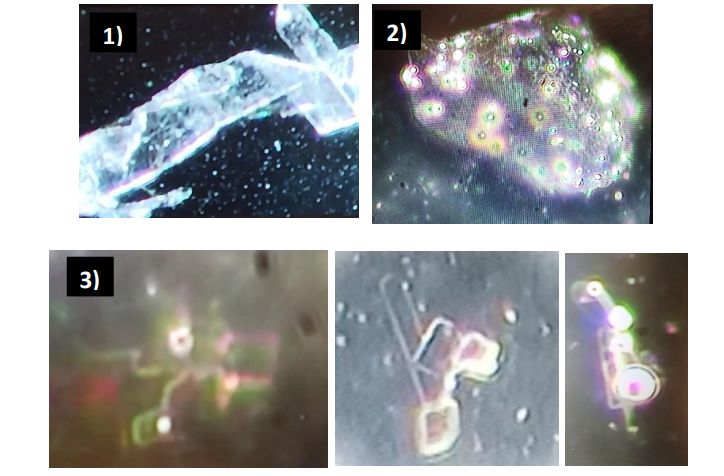
The Australian pathologists also studied the Pfizer vaccine itself using dark field and phase microscopy. The photos below are at 1000x magnification. They saw the similar anomalies 1) long thick folded ribbons, 2) large black crystals along with 3) a staggering amount of small aggregated rectangular and circular translucent and reflective particles that glow brightly under certain conditions. These do not afford with any previous experience of artifacts that have been seen.
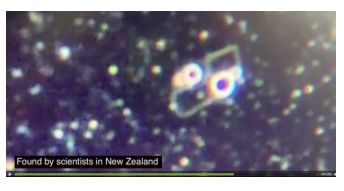
Dr Matt Shelton also detected the clusters of small rectangular and circular translucent structures in the Pfizer vaccine
With regard to blood samples:
“Blood samples now routinely exhibit severe rouleaux formations (stacking and clotting together). … They display unexpected foreign objects including 1) long folding crystalline sheets, 2) long tubular structures, 3) black crystals which attract and then destroy neutrophils. Figure 4 is at 1000x magnification and shows a small “spikey aggregate”. None of these structures have previously been seen or reported in the last 35 years of live blood analysis worldwide.”
[/gn_note] Annexure U
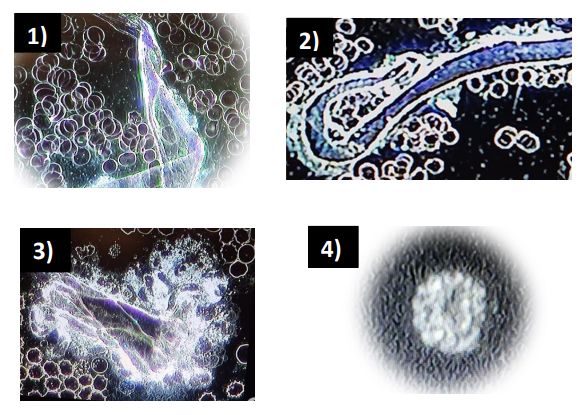
A group of Australian pathologists who specialise in Live Blood Analysis using dark field and phase microscopy have documented anomalies that have arisen since the vaccine rollout began in 2021. Blood samples now routinely exhibit severe rouleaux formations (stacking and clotting together). Figures 1-3 shown below are at 400x Magnification. They display unexpected foreign objects including 1) long folding crystalline sheets, 2) long tubular structures and 3) black crystals which attract and then destroy neutrophils. Figure 4 is at 1000x magnification and shows a small “spikey aggregate”. None of these structures have previously been seen or reported in the last 35 years of live blood analysis worldwide. The red blood cells seen in photos 1-3 measure approximately 6 microns in size. This gives an indication of the enormous size of these “contaminants” in the patients’ bloodstream by comparison.
Incredible as these claimed findings are, the CMN agrees that only thorough investigations of the vaccine contents can reassure or otherwise the public, who are increasingly aware of these findings through alternative media. In recent times, the practice of routinely examining blood films by pathology labs has been replaced by automated blood counts, so regular pathology laboratories may not be seeing these anomalies.
Therefore, will the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health recommend and provide funding for investigations using an array of microscopic techniques, including transmission electron microscopy (TEM) as above, into the contents of the vaccine vials and blood film analyses?
- This article in the International Journal of Vaccine Theory Practice and Research addresses the very real possibility that graphene and nanomaterials have been secretly used in the Covid vaccine products.
- [UK Lab] What’s in the Vials? (Moderna, Pfizer, AstraZeneca)
Reports of gene-based vaccine batch (lot) variability in risk of serious adverse events
While focussing on anomalies in the vaccines, the CMN is aware of research of the VAERS adverse event data that showed a statistically improbable variation in reports of adverse events according to batch (or in the US, ‘lot’) numbers.
The most benign explanation is there is poor quality assurance practices in the dosages and ingredients in these batches.
This anomaly might explain why some people have zero reaction at all to the gene-based vaccines, while others must take time off work or become seriously unwell, or die. Experienced virologist-vaccinologist, and original inventor of mRNA technology, Dr Robert Malone reports his own personal experience of no reaction after his first Moderna dose, but a life-threatening adverse reaction after his second dose (83). He checked the website (84) and found his first dose was from a batch with minimal reports to VAERS, but his second dose came from one of the 5% of batches that leads to greater than 90% of reports to VAERS.
A Dr James Hill has investigated this issue and draws some alarming hypotheses (85).
They’re operating so as to not run over each other. When company A is deploying lethal batches, companies B & C are deploying only harmless batches.
Knowledge of this issue is spreading via alternative media and causing concern. This is another area that warrants a high level official investigation.
Have the Chair of ATAGI, ATAGI committee members, the Secretary of Health, the CMO, the Deputy Secretary of the TGA, ACV committee members, or Delegate of the Secretary or TGA officers or the Minister of Health heard of this issue? Will you please institute a high level investigation of this issue?

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:
 Aussies
Aussies Or Buy me a Coffee (PayPal)

References

![[Tabletop] ‘A World At Risk’ W.H.O. “Prepare world for lethal Respiratory Pandemic & Universal Vaccine” Sept 2019](https://pennybutler.com/wp-content/uploads/2022/03/AWorldAtRisk-425x437.jpg)
