Autopsies: Evidence for Jab-Related Harm & Death. (Prof. Dr. Arne Burkhardt)
- Updated:1 year ago
- Reading Time:31Minutes
- Post Words:7819Words

Eight German pathologists, physicians and biologists and one physicist are working together looking at autopsies and biopsies of those suspected of dying from the Covid Shots. Prof. Arne Burkhardt shares the autopsy findings.
First Published: April 16, 2022 | Last updated: April 25, 2023
Target Organs & main Lesions:
- Vascular Lesions – Endothelium / Vessel wall
- Unidentified intravascular Material
- Spleen / Lymph nodes
- Heart
- Lung
- Brain
- Lymphocyte “Amok” in many Organs & Tissues
Professor Dr Arne Burkhart, German pathologist pathological examinations. (01) Download Dr Burkhardt’s tissue slides (PDF)
Histopathological reevaluation serious adverse events and deaths following COVID-19 vaccination
22nd January 2023 Rumble | Full presentation in English
Prof Arne Burkhardt – PANDEMIC STRATEGIES, LESSONS AND CONSEQUENCES, 21st- 22nd January 2023
- Short video extracts
Prof. Arne Burkhardt joined the World Council for Health “Understanding Vaccine Causation Conference” to share his presentation, “Evidence for Vaccine Related Harm and Death“
[00:00:06] Shabnam Palesa Mohamed: we’re moving on then to another speaker under our medical practice session. And he is Dr. Arne Burkhardt. Born in 1944 in Germany, a pathologist with more than 40 years diagnostic and teaching experience. He is the author of more than 150 original publications in international journals, currently engaged in autopsy studies of persons dying after taking the Covid vaccine.
[00:00:37] And Dr. Burkhart, before you deliver your talk to us, perhaps your thoughts first on why this conference on causation… bringing together multi-disciplinary experts is so important.
[00:00:50] Prof Burkhardt: Well, first of all I thank you very much for the invitation and the kind of introduction that you gave about what I have done in the past.
[00:01:00] I think it’s very, very, important to have an international communication on this subject because last year in may, April, I was confronted with some relatives of persons who died after vaccination. And I tried to establish a national registry of these persons dying.
[00:01:23] And I tried to get autopsies done in these persons, but the national associations of pathology here, didn’t reply to this request by myself. So when relatives continued to ask me, ‘ Where can I get some solution to this problem?‘ Finally I said I can examine these organ probes that have been taken during autopsy and we can try to get some other pathologists sent.
[00:01:52] Maybe I can show my first slide now, because if we talk about morphology about pathology, it’s not possible without looking at pictures and slides of tissues and cells.
[00:02:04] Shabnam Palesa Mohamed: Professor Burkhardt the topic is autopsies evidence for jab related harm and death. Dr. Burkhart, you have 15 to 20 minutes followed by 10 minutes of Q and A, the mic is yours.
[00:02:17] Prof Burkhardt: These are the most relevant data on our study. We have eight cooperating pathologists, physicians, biologists, and they are internationally from Germany and other European countries, and also some outside of Europe.
[00:02:33] So by now we have 30 autopsies and three biopsies from vaccinated persons. 15 cases have been evaluated in the step one that has reached Routine Histology. Three cases are in step two Advanced Methods. I will explain what I mean by this.
[00:02:52] And just to give you a rough Impression it’s seven men, eight women, 28 years to 95 years, Death seven days to six months after the last injection and vaccination, the typical vaccinations that are used in Germany.
[00:03:09] So one important fact is that most of these persons that we examined have not died in the hospital, but at home on the street in the car. And that is very important because in these cases, we can exclude that there are interference with therapeuticle measures like artificial respiration and things like that. So only four were in intensive care medicine before they died.
[00:03:37] We had 15 cases with autopsy elsewhere which we examined in step one. And all of these 15 cases were classified by the pathologist of legal medical persons who made the autopsy as natural and unclear. And the relatives insisted on a second opinion. And we in Reutlingen, in our group, looked at the specimens of the organs that were taken. Our follow up gave very probable correlation with the vaccination in five cases. Probable in seven. Unclear/ possible in two and no connections with only minimal changes we saw in one case.
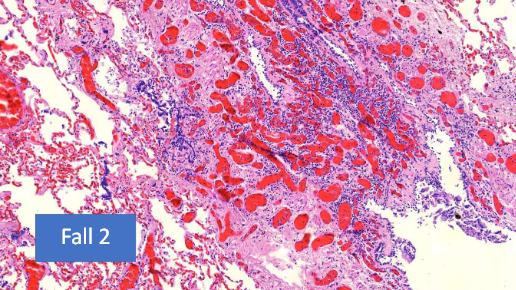
[00:04:21] So what were the organs where we saw lesions? The target organs and the main lesions in her space, Vascular Lesions. Not only to the small vessels, the Endothelium, but also to be Vesselwalls to the muscular and elastic wall components.
[00:04:39] In five cases we found unidentified intervascular material that might stem from the vaccination material. Then spleen and lymph nodes had changes. Heart, lung brain, and finally a phenomenon that we call Lymphocyte Amok. That means that we’ve found applications and nodular infiltration of lymphatic tissues and organs and tissues that are non glymphatic.
[00:05:09] So what are our methods? First of all, routine histological preparation with conventional stain and then Immunohistochemistry first send the markers for lymphocytes inflammatory cells. But mostly emphasis one of the aims of this study too, we try to demonstrate the spike protein in the organs and tissues set were damaged.
[00:05:36] And first of all of course, we examine the specificity of our antibody to a spike protein, and we did this in cell cultures and you can see here net negative control, positive control, and here a larger magnification. So it seems to have a very high specificity for this spike protein.
[00:05:59] And I will just show you a few examples of the tissue damage that I have listed before.
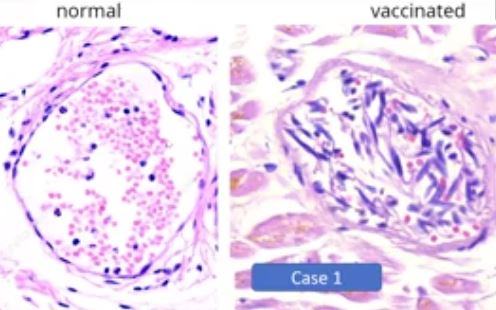
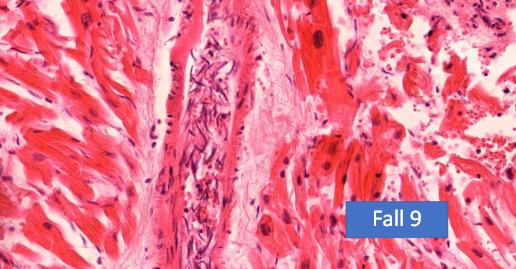
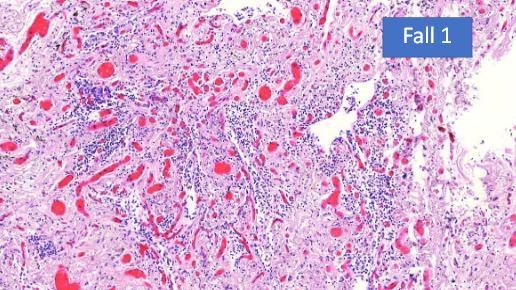
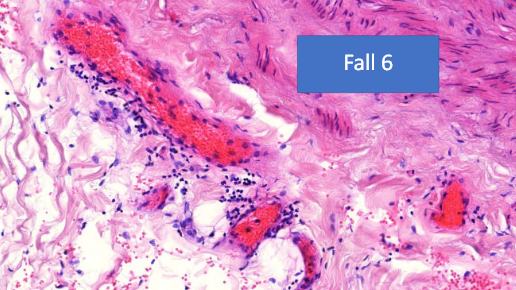
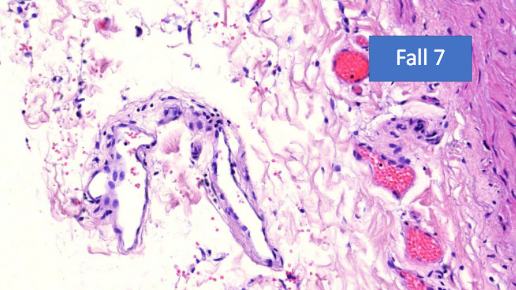
So here you can see a normal, small vessel, and you can see the Endothelium that is like a wallpaper and very small elongated spindle cell nuclei. And here in one of the cases, you can see that the Endothelium is in the lumen. And it is in there mixed with Lymphocytes and Erythrocytes and the nuclei is swollen.
[00:06:32] So in some cases the small vessels even are completely destroyed by inflammatory infiltrates, mostly Lymphocytes. And this proves to me that it is an intravital reaction and not an autorhythmic phenomenon caused by degredation after death.
[00:06:51] So we get the spike protein, immunohistochemistry on these cases and we see, you see here a very marked and specific, eh, the mark of the endothelium in these patients. And not only in the small vessels, but also in the smaller arteries, you can see it in the inner part of the vessel. And you can see here there’s decemated endothelial cells.
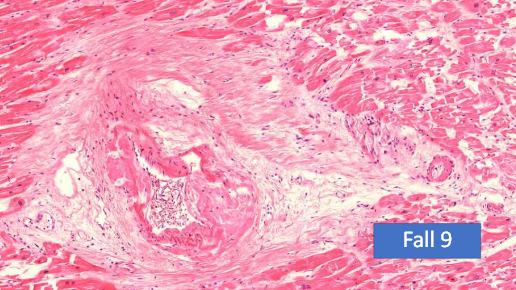
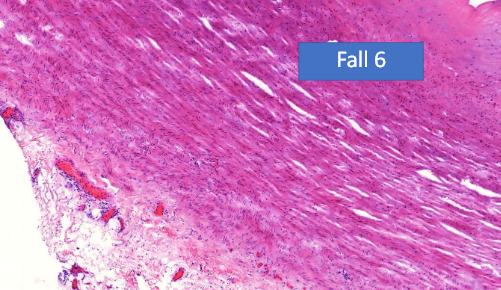
[00:07:21] So not as I said, not only the smaller vessels were affected, but also the aorta and the larger arteries and two cases have died of a ruptured artery. And actually we found arteriosclerotic changes, but as you see here, it’s not very pronounced. But you can see inflammatory changes around in the deep layers of this aorta and also you can see some disturbance of structure of the smooth muscle and the elastic fibers. And if you have a higher magnification, you can see these small areas where the elastic fibers and smooth muscles are destroyed.
[00:08:09] And again, lymphocytic infiltration proving that it was an intravital process. And here another case. We found it in, in five cases so this cannot be a coincidence. And we did the spike protein, and you find a marked positive expermeation of spike protein in the myofibroblasts of the arterial wall. This is the aorta. And also in the [unintelligible], you can see very strong expression of spike protein in these areas. And this I think is a very important finding.
[00:08:54] So how often did we see this vasculitis, this endovasculitis or some call it endothelitis, in 11 cases with focal lymphocytic infiltration, then vasculitis paravasculitis in 10 cases, fokal media-necrosis in six cases, and thrombosis caused on this area in two cases.
[00:09:19] So similar lesions are caused by toxins and drugs cytostatic drugs, and in some food poisoning like Lathyrism. And so we think also here a toxic element, the spike protein might be the causative agent.
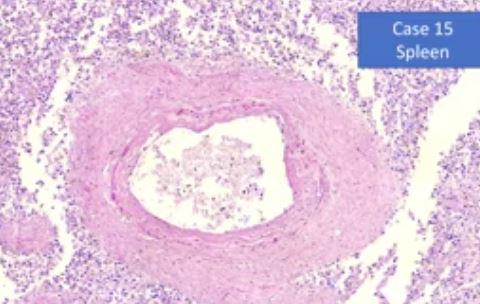
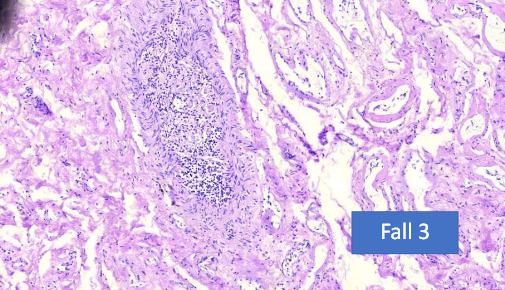
[00:09:39] Now another, other lesions that we saw in the spleen. We first overlooked, but the more we looked, the more we found it. And this is one phenomenon that is known as onion-skin, arteritis of the spleen, which is seen in some autoimmune diseases like lupus erythematosus.
[00:10:01] And in the course of these arteriolitis we saw focal destruction of follicular arteries in the spleen and products of the lymphatics follicles. Now, first of all, this picture is an overview of two organs in one paraffin dock. You can see here, the liver and here, the spleen. And so both organs have had the same preparation, the same fixation and everything.
[00:10:33] So you can see easily that the liver is practically non-reactive. You can see some small vessels, the epithelium is positive, but the liver itself is negative. And then in contradiction, the spleen has a very pronounced mark around the vessels and small arterials.
This is a liver now, and you can see the liver cells itself are negative, but the small vessels, the capillaries have a strong, positive reaction of the endothelium.
[00:11:10] And this is this reaction that is called the onion-skin phenomenon, which is seen in some autoimmune diseases.
You can see the wall of the artery is split up in, in a way. And also here we can show, as we saw on the overview that there’s a strong reaction for the spike protein.
[00:11:35] And this is a phenomenon that none of the pathologists that I work together have ever seen before.
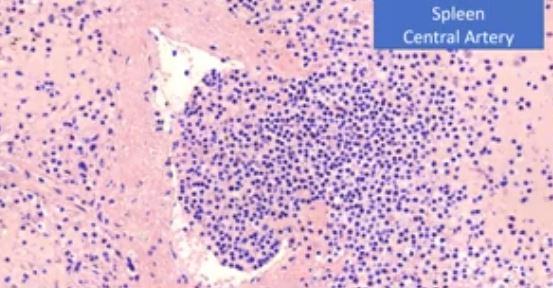
This is the small artery in the spleen, and you can see the wall has a focal defect and the lymphatic tissue is protruding into the vessel. So it also changes in the lymph nodes. We have seen a case of a pseudolymphoma, as I can show you here. It’s at least three centimeter large. And then in another case, we saw a focal central infarct of the lymph nodes.
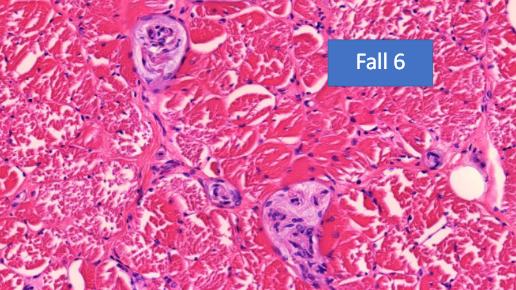
[00:12:15] Now the myocarditis is now I think it’s internationally known that it is a side effect of vaccination.
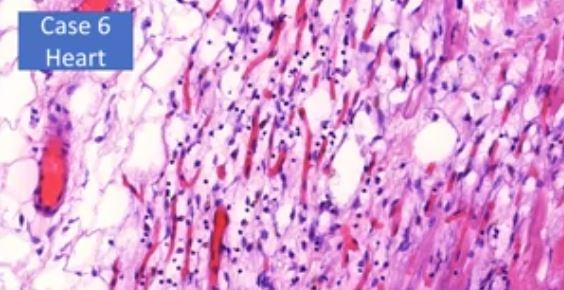
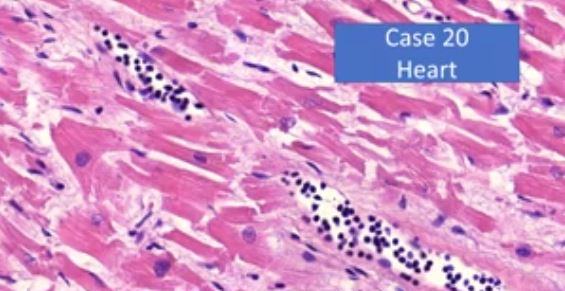
And you can see that in our cases, we saw these lymphocytes marching up in the small vessels here. You can see the intact muscular fibers. And in this case, you can see that they are destroyed by the lymphocytes that are infiltrating in contradiction to the infarction to the true infarct of the cardiac muscles. Do not see granulocytes in these areas. Only very few when some macrophages, of course.
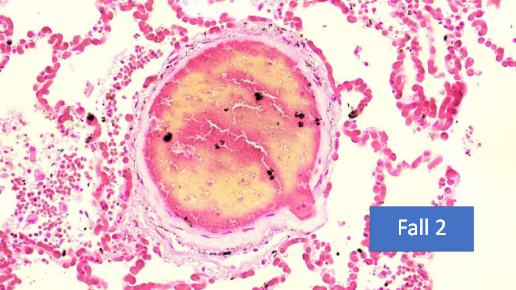
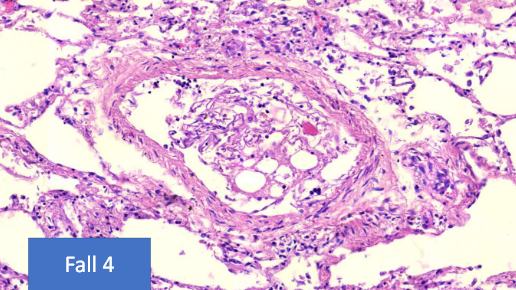
So we come to the lung here, you see a normal lung. You can see here all the white areas of the lung alveoli.


[00:13:02] And what we found are very pronounced changes in which you might call a lymphocytic alveolitis, lymphocytic interstitial pneumonia. And you can see that only very few areas where there are still aveoli. These, the infiltration is mostly T lymphocytes, CD3 positive.
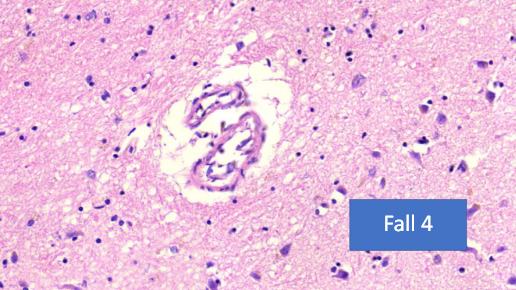
[00:13:30] Very important are the changes that we found in the brain.
We found
- Transfection-associated Encephalitis
- Lymphocytic infiltration and focal destruction of intracerebral and arachnoidal blood vessels
- Subarachnoidal haemorrhage without Aneurysm (in young people)
- Focal lymphocytic infiltration of the Dura mater.
- In one case Necrosis of the Hypophysis (partial necrosis of the Hypophysis).
[00:14:03] Now this, just for those that are not familiar, this is Dura mater. And here we found infiltration by lymphocytes. This is the, the, arachnoidea where we found a perivascular inflammation, and we also found it in the brain. This is Dura mater, you can see this focal infiltration by lymphocytes. This young 26 year old died of hemorrhage. No, no aneurysm, and you can see that the vessels in the brain and in the [inaudible] have a focal lymphocytic infiltration, and, probably that caused a rupture, also infiltration by lymphocytes.
[00:14:52] And this is a case of the encephalitis, which we observed. And in this case, we could demonstrate a spike protein, again, in the smaller vessels. And here, a small artery here, very pronounced, positive reaction. Another area where you can see this definitely and very, clear positive cells. It’s mostly in the small vessels, but also in some neural cells.
[00:15:26] And now in a phenomenon that we call the Lymphocyte – Amok, which is a lymphocyte accumulation in lymphocyte predominant tissue destruction outside of the myocardium and the lung where I’ve already demonstrated is. It’s definitely the danger of a prolonged auto immune disease.
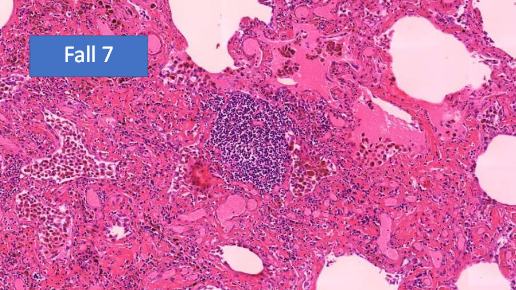
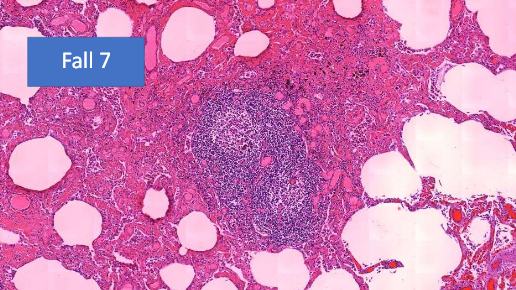
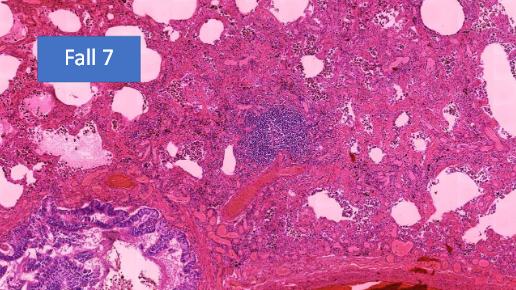
[00:15:49] In this, we found in non lymphatic organs and tissues. There are some autoimmune diseases which are related to this phenomenon. And this is in the lung.
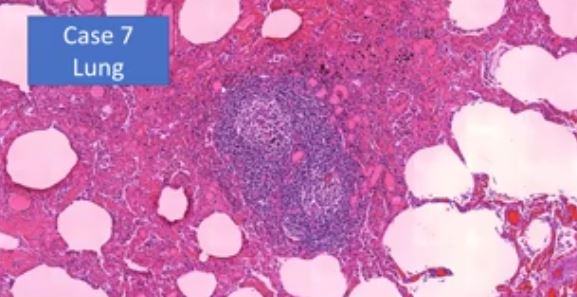
In the lung sometimes you find a small lymphocytic elements, but I have never seen before [inaudible] quasi lymph node with reaction centers and activation.
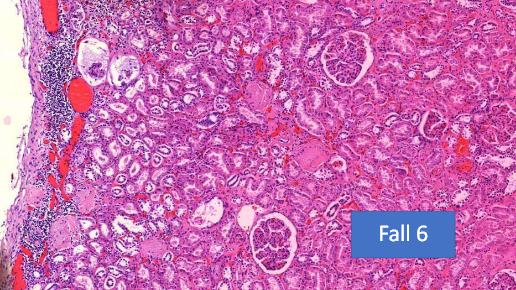
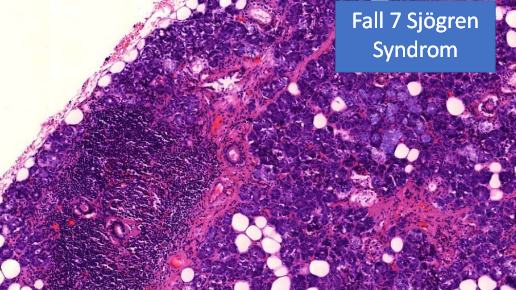
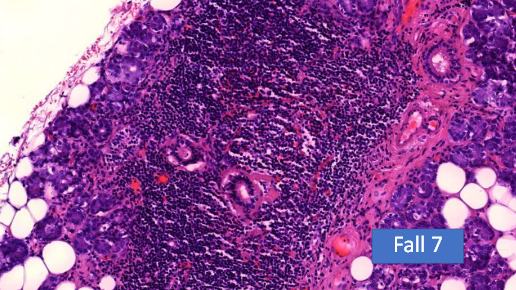
[00:16:13] And this is the frequency that we found of these lymphocytic infiltrations, the thyroid glands, the salivary glands. And by the way, of course, we found this in two cases, but we only had these organ specimens in two cases. So it was found in 100% of the cases that we examined. So in the aorta, I showed you before, skin liver, kidney, lymphocytic pyelonephritis, nephritis, in the testis, in one case, and in the Dura, I showed you this phenomenon.
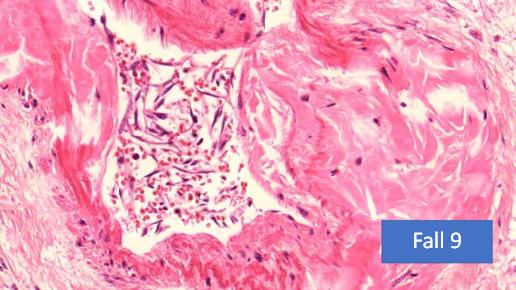
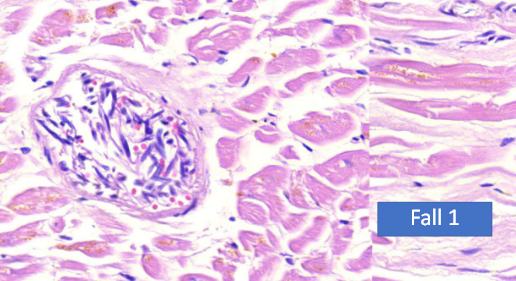
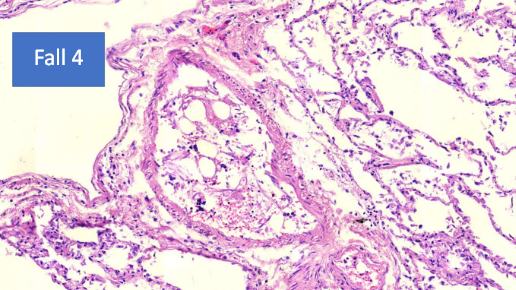
[00:16:49] So these are the organ changes. And just as the last lesions that I would like to show you is unidentified foreign material in the vessels, especially in the spleen vessels. And this is something that we could not identify. No pathologists that have looked at it knows what it is. First we saw these cells but they have an inner structure like [inaudible] and then we thought it might have been a contrast material but this patient died at home and was not in the hospital for a long time.
[00:17:29] So our theory is that these are the nanolipid particles, which when they come into the body and a warmed up which coalesce and form larger particles that might at one point stick in the system, in the vessel system. And this was one case in the spleen, and this is another. This one was only a few days, and this is after some longer period of time. I might add that this is a coincidental finding because this was not macroscopicly seen, but we had it by coincidence in our sections.
[00:18:11] I will show you a case report. Over natural death uncovered as caused by vaccination-induced vasculitis of the coronary artery.
[00:18:21] It was a 50 year old man, two vaccinations, and he died 123 days after the second vaccination. And there was no doubt this was myocardial infarct. The primary autopsy was [inaudible]. They saw a discoloration of the cardiao muscle and said, well, yes, he died of a myocardial infarct but then we did histology of the coronary artery and we found these changes.
[00:18:59] And in addition, in the muscle we found the myocarditis, as we found typically in the other cases, as I have shown. Now this is the coronary artery and yes, you see it’s clearly there. Is thrombus formation inside. And yes, there are arteriosclerotic changes. But look at these areas and here around the vessel. There’s definitely inflammatory reaction.
[00:19:26] And you can see these disturbance of texture of the smooth muscle and the myofibroblasts here and you can see also some discrete lymphocytic infiltration. And then around the vessel, around the vessel, there’s this dense lymphocytic infiltration. So we concluded that the vessel, the coronary artery, had an inflammation induced by the vaccination, by the spike protein. And the thombus was built on the ground of these inflammatory changes and led to be infarct, which definitely was present.
[00:20:15] But also the fact that there was a concomitant, myocarditis, very strong evidence that this secondary, because of the vaccination. And for many, we spent many hours looking at all these slides. And for a long time we were thinking, well, we are chasing a Phantom and we looked at each other and ask each other, do you see this? Do you see this? Is this real?
[00:20:45] And we are now at a point, and especially after we could prove the presence of spike protein for months after vaccination, we are come to the conclusion, no, we are not chasing a Phantom. Further studies are necessary and I think it’s a very exciting field that we are coming to, but also a very depressing and very scary phenomenon. Thank you.
[00:21:13] Shabnam Palesa Mohamed: Thank you, professor Arne Burkhart, for your incredible contribution to health science, and humanity. We are slightly over time, but I believe everyone is really appreciating this conference on causation. So I’m going to ask my colleague Mark Trozzi to take two questions for the professor before we hand the mic over to Dr.
[00:21:32] Ryan Cole, who will be talking to us about the proof is in the blood causation in pathology. Mark?
[00:21:41] Dr. Mark Trozzi: Thanks, Shabnam. Thanks very much Dr. Burkhart. I’ll be brief in my admiration and thanks to you, but I could go to great length in that, but thank you for showing us in unquestionable terms, what is seen through the microscope and what has been happening to our fellow humans who have been given these injections.
[00:21:58] So I’m going to pick two questions. One is very sweet and it’s an anonymous attendee who says, “Professor Burkhart, do I understand that you came out of retirement to help us, the people of the world in need?”
[00:22:10] Prof Burkhardt: Well, actually, I was just retiring a few months before I started to study. I gave back my license for the health insurance in April last year. And in May, I was contacted and they asked me if I would do this study. And I, by the way, I also have some consulting contracts with some other laboratories.
[00:22:39] So I’m not retired in the way that I am not active anymore, but I’m retired in the sense that I am not responsible to anybody and that I cannot be thrown out of my job. I’m independent.
[00:22:58] Dr. Mark Trozzi: Thank you very much from all of us present and otherwise. One other question comes from [inaudible]. By the way, Dr. Burkhardt, I hope you have the time after. There’s some great questions. Lot of people keen to ask a question.
[00:23:10] Please forgive me, those that I was not able to get to, but this person is asking about toxicology test. What types tests on body fluids should a forensic toxicology laboratory do to prove death due to vaccines? Histology is usually requested by pathologists and clinical lab tests will test for traponin in living people, usually that this is not done in forensic toxicology laboratories. So I think in summary, for people that don’t have access to histology and autopsy, do you see there being laboratory tests to help prove causation?
[00:23:45] Prof Burkhardt: Well, I’m a pathologist and I’m not doing laboratory tests on blood or serum or anything. But if there are any lesions, I recommend to take a biopsy and if there are lesions found in the microscope to do immunohistochemistry in the future. So, maybe Ryan Cole can answer this better than I.
[00:24:11] Dr. Mark Trozzi: You’ve brought forth the powerful point that there’s no replacement for the histology and proper staining. So thanks for your leadership.
[00:24:17] Shabnam Palesa Mohamed: Thank you, Professor Arne Burkhardt. We are grateful for your time and your commitment, and we look forward to you perhaps spending more time with us in Understanding Vaccine Causation Conference Number Two. Thank you very much for joining us from Germany.
Dr. Arne Burkhardt MD: Expectations Fulfilled – The Scientific Evidence I Symposium 3 I Doctors For Covid Ethics – February 18, 2022
0:00:00.4 Sucharit Bhakdi: And the top of the story is going to come now, when Arne Burkhardt is going to show you that the first fears that we had, were good founded, and that there is organ damage that is being produced by vessel damage and by immune attack of your tissues after you receive this vaccine. So Arne Burkhardt, thank you for coming again, and we are looking very much forward to see your results today.
0:00:37.0 Arne Burkhardt: Yes, thank you for the invitation. I would like to give a short overview of what we are doing in Voitting since about the middle of last year when relatives came to me and asked me to investigate why some of their relatives died and they suspected a connection with the vaccination. And by now, we are all in all eight pathologists, physicians and biologists and one physicist that are engaged in this study where we look at autopsies and specimens taken from living person’s biopsies, and we have now 30 autopsies and four biopsies, and these were examined by routine microscopy, which is done in 15 cases by now, and we have three that have been examined by advanced methods that I will show in the next slides.
0:02:09.0 AB: Next, please. Next slide. So here you have the characteristic of these 15 initial cases, we had seven males, eight females, the time of death was seven days to six months after the last injection. Age range was 28 to 95, and you can see the different kinds of vaccinations that were used here. Most often was Pfizer and Moderna. Next. So we looked at the specimens that were taken by pathologists and forensic pathologists that had performed the autopsy and we received the specimens and we looked at them and in all of these cases, there was no suspicion that this could have had a connection with vaccination. Only their relatives had this suspicion. And so the forensic medicine did no further examinations, especially they did no histological examination.
0:03:40.6 AB: And in our second opinion, we came to the conclusion that there were definitely… In mostly all cases, there were some changes that we… Because we’re seeing regularly, we contributed to changes caused by the vaccination. And these, as we think, contributed to the multifactorial deaths occurrence in these patients, and we think it was very likely in five cases, likely in seven, possible in two further and excluded, that means only mild changes, in one.
0:04:30.6 AB: Please, next. Important is the fact that most of the deaths that we examined, it… Died suddenly at home or on the street. Important, only a few did die in the hospital, and so we can exclude therapeutic changes in, for example, for lung because if you have some artificial respiration, then of course, in the lung you don’t see any effects of the vaccination anymore, but only effects of the artificial respiration.
0:05:19.9 AB: Next slide. Next. And this is just to show you that practically we found changes in all organs in the first place in the blood vessel. For one, in the innermost layer, the endothelium, and then in the vessel walls of the larger vessels, we found unidentified intervascular material which might have originated from the injection. We saw marked changes in the spleen and lymph nodes, and then in the heart, lung, brain, and finally, what you might call a lymphocyte, amok or lymphocytosis in many organs and tissues, that are not lymphatic tissue like lymph nodes or spleen. And which, if we see them, usually are correlated to autoimmune diseases. Next slide.
0:06:30.4 AB: So, based… The methods used might not be familiar to all of this… So I listed them here. Routine histological preparation with conventional stains and different special stains, then immunohistochemistry. Different antibodies against the cells of inflammation. Different subtypes of lymphocytes and the most important is that we developed an immunohistochemical method to show SARS-CoV-2 virus spike protein, subunit 1 in the tissues and we found them in many of the lesions that we have seen. Next slide, please.
0:07:26.7 AB: So just for those who’ve never seen a picture or histological slides. You see here a normal liver and you can see normally if we just cut it… It does not have any colour but we colour it so the nuclei are the small dots that are dark or black, and the cytoplasm is red and you can see sometimes some inter-cytoplasmic features and changes.
0:08:03.0 AB: Next. So first of all, and I think most important are the changes in the vessels because the vessels are practically in all organs, there are only very few that do not have vessels like the lens of the eye and et cetera. So you can see normally the endothelium is like a wallpaper surrounding the inner of the small vessels and in these cases… In the cases of the vaccinated, we found that these were desquamated from the nuclei swollen and they are intermixed with erythrocytes. Now, this phenomenon, sometimes you see as a cause of autolysis, that means after the death, but… Please next slide. But we definitely in many cases saw that actually these vessels were destroyed. If you look closely, these spindle cells that you see here, are the endothelium that has been damaged and then there’s a lymphocytic infiltration which definitely proves this is an intravital process.
0:09:31.8 AB: Next slide. So we were interested in how… If this was related to the spike protein, and we developed this method of showing that the spike protein for those who have not worked with immunohistochemistry, this is a small scheme to show you how. So actually, there are some antibodies that are bound to what you are searching for, and finally you have something with colour. And so the colour is demonstrated in the cells, and here you can see how they are positive in some cells. And we first did some examinations in cell cultures. Next… Next slide.
0:10:32.1 AB: The cell cultures… You see we had cell cultures that were negative controls and others that were affected with cormirnaty here you don’t see a positive cells here, you can see the positive cells. And after that we applied it to our specimens and we have some… About six cases now.
0:10:57.3 AB: Next. Next slide. And here you can see the small vessels. Here, you can see the endothelium with a marked positive and distinct colouration as I showed you, and here, this brown is in a small arteriole and you can see it is definitely limited to the inner part of this vessel.
[pause]
0:12:07.2 AB: I don’t know how this happened. Okay, excuse me. Okay, as I said, we found changes not only in the small vessels, in the capillaries, but most alarming in the larger vessels, especially in the aorta, and actually we have two cases now, that died of rapture of the aorta. And we found these changes in… Normally, the aorta has regular layers of smooth muscles and elastic fibers, and, no lymphocytic infiltration, and you can see here, this is the inside where the blood flows, and this is the appendix, the vasa vasorum and you can see there’s a dense lymphatic infiltration, and you can see some textures, irregularities here in the wall. Next slide. Next slide please.
0:13:16.4 AB: And, you can see in a higher magnification, these small lesions… And again, the fact that there are lymphocytes in the vicinity, proves that this is a vital process, and not something that is caused by autolysis or after death. And actually, when we first saw this in the first case, we thought… We looked at each other and said, “Well, this man had a problem with his aorta, it’s his vessels, but, when we had the second case, and the third case, and actually we have five cases now, not all ruptured, only two ruptured, but the others still with this section, we definitely came to the conclusion that this was connected with the vaccination. Next slide. And… So we had the suspicion that this damage of the arterial and aorta wall, is caused by the vaccine, and actually as you may see here, especially here around the vasa vasaorum there’s a dense mark and coloration of these cells here, and also the myofibroblasts in the aortic walls are definitely a distinctly positive. So, we could show that there’s a spike protein in here. What we cannot decide, is whether it was produced here or whether it was just taken up by the cells, but definitely it did damage to the cells. Next slide. Next slide, please.
0:15:07.2 AB: And now, how often did we see this… I have listed the cases here, so endothelialitis or lesions of the small vessels and the filum, 11 cases, and vasculitis, perivasculitis of the larger arteries in 10 cases, and focal vessel evolved necrosis with inflammatory reactions, in six cases… Sorry, I said five cases before, but [chuckle] when I wrote this, we had another case, every day there’s one more case, it mostly is. In two cases, we had additional thrombosis in these areas. Next, next, next slide. And for those who are not accustomed to histological slides, and may think, well, “What the hell is going on in these slides? What does this interest me?”
0:16:16.2 AB: This is a lady 42 years old. She ran… She did participate in marathon, walks now runs. In the past, even before vaccination, and she developed severe problems with her legs and feet, and actually now she’s lying in bed, and can hardly go to the toilet. So this is absolutely frightening, I think, 42 years old former marathon participant in marathon runs, until… Definitely before the vaccination. Next slide. So the spleen and the lymphatic organs, the lymph nodes, especially have special changes, and some of these changes we see in autoimmune diseases, like the so-called “Onion Skin Inflammation” of the central arteries, and what we, as I think found for the first time… And all the pathologists that participated, and to whom I presented this which are about 50 now, have never seen this phenomenon before, so… Next slide, first, the so-called “Onion Skin.” Next slide. No. Okay, excuse me. This is an immune histochemical overview of two organs in the same paraffin block. I will come to the onion skin lesion, after that. You can see here, the liver is practically non-reactant, it is… But you can see in… Close to the spleen, which is in the upper region of the picture, definitely and very marked expression, especially in the vessels, and, also in the spleen… In the liver, the small vessels are positive, but here also larger arterial walls are definitely and very explicit positive, and next slide.
0:18:54.3 AB: First, if you look at the liver, you can see the liver cells are negative, this is just a little bit non-specific staining, but the small endothelium in the liver is definitely positive, next slide. In the spleen we found lesions in these three areas, I had mentioned… I mentioned already the foreign material in the arteries and the activation of the red pulp, but especially the central arteries, which are here in these areas affected. Next slide. Next. And this is a phenomenon which is known to pathologists as a onion-skin inflammation of spleen arteries, you can see, this is not a regular arterial wall, but it has some… Like an onion skin, this is especially seen in lupus erythematosus which is a well-known and not so good autoimmune disease. Next slide. End. Next slide. And these onion-skin lesions actually, we find a strong expression of spike proteins, which is marked, very marked, in the whole spleen you find some… Some positive staining, but this is absolutely special and very clear. Next slide.
0:20:45.2 AB: And this is a phenomenon that I think nobody has ever seen before, this is the central artery, here, you can see the wall. This is the red. And then you see here is split in the wall and the wall and the lymphatic tissue is invading a rupture into the artery. Now, the explanation may be that when lymphatic tissue is perforating, of course, it exerts pressure and in contradiction to spleens of some animals, the spleen of a human being, has a capsule that contains only very little smooth muscle, so it cannot expand, so if there’s an increased pressure and the central arteries of the spleen have lesions, this pressure leads to this phenomenon. Next slide. And the lymph nodes are definitely enlarged, you can see here it’s about 3 cm and it shows what we call a pseudolymphoma.
0:22:13.4 AB: Next slide. And in other cases, this is a normal lymph node, you can see these lymph follicles and here we have a central infarction of the lymph nodes, now this is seldom seen, it’s described by some Japanese authors and it is also probably associated with vessel… With small vessel or thrombotic events in small vessels of the lymph nodes. Next slide. Now, I think the occurrence of myocarditis by now is internationally very known. Here, you can see a normal heart and here you can see these lymphocytes marching up into the… In-between the muscle fibers. Next slide. You can see that in some cases, there’s a destruction of these cells and in contradiction to normal infarction, here lymphocytes predominate and some macrophages, but only very few polymorphonuclear granulocytes. Next. Next slide.
0:23:45.9 AB: And just one picture of the lung, this is a normal lung, you can see these air-filled alveoli and you can see after vaccination and these were people that, these people were not artificial respiratory… Respiration in the hospital, and you can see, there’s only very few air-filled spaces anymore and a definite lymphocytic infiltration and again, not polymorphonuclear granulocytes like in bacterial pneumonia. Next. Next slide. And if you do immunohistochemistry, these are CD3-positive T-lymphocytes, they are not B-lymphocytes as in banal inflammation. Next slide. And we come to the lesions of the brain and the surrounding tissue and we have lesions in the dura mater, we have lesions in the arachnoid area and also in the brain tissue.
0:25:07.9 AB: And next slide will show you a case. Next slide. They show you the main findings, so we see a transfection associated encephalitis, lymphocytic infiltration and destruction of intracerebral and arachnoid blood vessels, subarachnoid bleeding without an arrhythmia which is the usual case of this lesion. Focal lymphocytic infiltration of the dura mater and necrosis of the hypophyseal glands in one case we found that. Next. Next. This is the lymphocytic infiltration of the dura mater in a 26-year-old patient and you can see this is a normal straight fibre tissue and you can see here definitely lymphocytic infiltration. Next.
0:26:19.5 AB: And small vessels in the brain, you can see here, this is a very delicate wall actually, but there are some lymphocytes in there and so this is definitely vasculitis, inflammation of the small vessels. Next. Okay, this is what we saw in the brain and now I will just show you one additional case report of a necrotising encephalitis of a 76-year-old man. You see the data here and here what we found by autopsy. Next slide shows you the lesions in the brain. You can see there’s a necrosis and you see they’re definitely inflammatory cells. Next. And again, we showed spiked protein mainly in the vessels, here, here, but also in some cases in the neural cells, some cells, very few, but mostly in the vessels. Next slide.
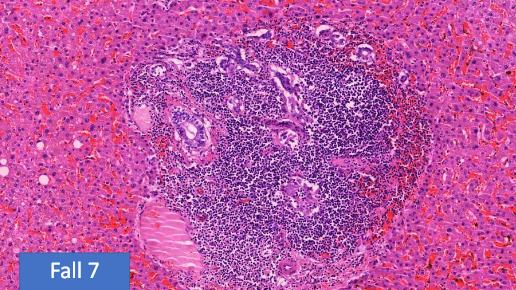
0:27:51.8 AB: Here you can see the, above, the positive mark in neural cells. This might be an endothelium but these are neural cells. Next slide. And finally, this phenomenon that we call lymphocyte amok, this is the accumulation and tissue destruction by lymphocytes in non-lymphatic organs, which is also, again, a phenomenon seen in auto immune diseases. Next slide. Just a few examples, I could show you endless pictures, but here you can see how often we found it. Actually usually like thyroid glands, we found it in two cases but actually we only had the thyroid glands in two cases. So we had it in all cases that we examined the same as in salivary glands, the vessels we already saw them in the skin, liver, kidney, testes and dura mater I showed you. Next.
0:29:08.1 AB: And again, a normal lymph node and here you can see the lung and you can see that in the lung there’s not only a lymphocytic infiltration of nodular characteristic, but there’s definitely a germinal center formation, so actually a small lymph node inside the lung. Next slide. And this is just an overview of the thyroid glands and you can see these dark areas are all lymphocytic infiltrations, so this is what they call thyroiditis Hashimoto. Next slide. And this is the strange material that we found in the vessels, which we, in some cases that we have not identified yet, but I just wanted to show you. I don’t want to speculate here. Next.
0:30:10.0 AB: Just one final case report to the autopsies, there’s this case, 25, which was declared as a natural death, because there was definitely infarction of the cardiac muscle. A 50-year-old man, he was vaccinated and also during the autopsy, there was clearly an infarct found, also an arteriosclerosis but then histology was done. And next slide. We found, first of all, a lymphocytic myocarditis in addition to the infarction and then we examined the coronary artery. Excuse me, one back please.
0:31:11.6 AB: And you can see definitely there is a thrombotic occlusion which of course caused the infarction, but then you can see that this wall has definitely atherosclerotic changes, there’s no doubt about it. But if you go into the deeper tissue here, you can see there’s some structure disruption and especially around the wall, in the periphery, around the wall there are dense lymphocytic infiltrations and this is shown in the next slide. So you can see here, these small lesions, this may be atherosclerotic, I’m not sure, but this definitely has nothing to do with arteriosclerosis and you see the lymphocytes in the vicinity of the vessel. Next slide.
0:32:10.1 AB: Yeah with a stronger magnification you can see these cuff-like lymphocytic infiltration of the vessel and also in the vicinity. Next slide. So I will come to the few specimens that we examine of living person, examination of bioptic specimens, we had an appendectomy, a bronchial biopsy and excision of skin lesions. Next. This is atypical appendicitis and actually inside the appendix there was, as always there was some inflammation, but not very much, but there was marked inflammation in the fatty tissue around the appendix or periappendicitis. Next slide. And we could show, again, weak but definitely positive expression of a spike protein in these vessels that are located in this inflammation. Next slide. Here, a larger magnification and you see this is really specific. Next. Next slide.
0:33:46.7 AB: So this is a bronchial biopsy of nine months after Corona vaccination of a 26-year-old man who had bronchoscopy because he had difficulties with breaths. He had palpitations, blood pressure irregularities, pain in the thorax and fear of suffocation, so they made a bronchoscopy and in the report they say, “Well it was all normal, nothing special.” And they recommended this young man should go to the psychiatrist because of this sensations. Next. Next slide. Shows you the bronchial mucosa and you see a definitely inflammation here. I will not show you there were dense infiltrates of eosinophilic granulocytes. What is important here is, you see in between the epithelial cells, there are these dendritic cells that are probably related to immuno-recognition. And next slide shows you that these dendritic cells are definitely positively stained by the spike protein. And this is a very unusual finding in my opinion.
0:35:27.9 AB: And also there was a weak expression of spike protein in the endothelium, but not very much. Next slide. And finally a skin biopsy and here we found these were a little bit granulomatous inflammation, very expressed, expressive, very definite inflammation. This might be a small necrosis, I’m not sure. We have to make further stains and we didn’t have immunohistochemistry in this case, but next slide shows you that there are some very strange cells in there, which were in my opinion, they remind me of Hodgkin cells, which of course are also modulated and deregulated lymphocytic elements.
0:36:30.0 AB: So I think this is… Please next… At least the next and last slide I think… Well, we actually… We were often looking at each other when we’re sitting on the table microscope and we ask each other, “Well do you see this? Is this really true, could this be?” And we were always thinking, “Well, we might be chasing a phantom.” But we definitely have come to the conclusion, “No, this is… These are real and very alarming lesions that we found and further studies are necessary and provocative.” And I think what we have now should be brought to the public in spite of the fact that, of course, not all conditions of scientific proof are given. But I think we have, we are almost at this point, thank you.
0:37:40.8 Sucharit Bhakdi: Thank you very much Arne. Arne, what you show is so horrifying and so alarming that even politicians should be able to realize that something, it’s not serious, it’s… There’s no word to express this. If they don’t start doing something, they’re going to be in real trouble because let us state this very clearly. These agents are in experimental stage of use. There is an iron law saying that if you are introducing a medicine or an agent into the body of a person under experimental conditions, then you must always assume that if anything happens to the patient, it is the new agent that is causing it. And you are obliged to go and find out. You are not allowed to turn away, you are not allowed to turn away. And you do not expect others to come to do the work that you are supposed to do. Now Arne has been doing work that the authorities, the governments, the protagonists and the instigators of these vaccines were under duty to do and they did not. And whether or not the findings that you have brought up are conclusive or not, is absolutely immaterial, but they’re already damning as the stand.
Vaccine related brain damage – Josef Thoma MD PhD discusses & explains the pathologists findings:
The video is dealing with brain damages caused by the corona vaccination. It discusses and explains the dramatic findings made by the German pathologists A. Burkhardt and W. Lang
Autoimmune

Lymphocytosis
Sjögren syndrome
Myocarditis
Vasculitis
Relevant Links:
- Understanding Vaccine Causation Conference – Prof Arne Burkhardt “Understanding Vaccine Causation Conference” – Broadcast Feb 6, 2022
- Doctors for Covid Ethics and UK Column Symposium – Prof. Arne Burkhardt MD: “COVID-19 “vaccines” can induce self-destruction“ – Broadcast Dec 10, 2021
- Doctors for Covid Ethics Symposium III – Prof. Arne Burkhardt MD with Prof. Sucharit Bhakdi MD “Expectations Fulfilled: The Scientific Evidence Presentation” – Broadcast Feb 18, 2022
- evidence of the damage done by COVID vaccines to small blood vessels. The endothelium – the ‘wallpaper’ of the blood vessels – is destroyed by invading lymphocytes. The destruction will result in blood clotting.
- evidence of inflammation and destruction caused by the vaccines in the wall of the aorta, the largest artery in the human body. He has meanwhile observed five such cases, two of which resulted in a catastrophic failure and rupture of this vessel.
- Notes and recommendations for conducting post-mortem examination (autopsy) of persons deceased in connection with COVID vaccination – Updated Mar 20, 2022 – PDF
- On COVID vaccines: why they cannot work, and irrefutable evidence of their causative role in deaths after vaccination – Dec 15, 2021 – PDF
- First time detection of the vaccine spike protein in a person who died after vaccination against Covid-19.- Mar 11, 2022
- German Parliament Hearing on Mar 21, 2022 – Prof. Arne Burkhardt (English Subtitles)
- Grand Jury Day 4 | Prof. Arne Burkhardt (in English)
- First case of postmortem study in a patient vaccinated against SARS-CoV-2
- Professor Arne Burkhardt (Walter Lang)
- https://twitter.com/ArneBurkhardt
- https://prabook.com/web/arne.burkhardt/42818
- https://swprs.org/covid-vaccine-injuries-the-german-pathologists-findings/
- Original German language presentation https://www.youtube.com/watch?v=jLJXL3YlHKE
- Link page to translated version http://docs.shortxxvids.com/burkhardt_analysis.html
- 2nd conference on vaccine adverse events (English translation) https://odysee.com/@LongXXvids:c/Prof-Arne-Burkhardt—2nd-Vax-Injury-Conference—Part-1:1?&sunset=lbrytv
- The same document in pdf format is available here
- Two unrolled Twitter Threads (in PDF format) that provide a simple exposition of Prof. Burkhardt’s findings.
- Thread 1
- Thread 2
- Short video extracts
What’s In the Vials?

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:


References[+]
Truth-seeker, ever-questioning, ever-learning, ever-researching, ever delving further and deeper, ever trying to 'figure it out'. This site is a legacy of sorts, a place to collect thoughts, notes, book summaries, & random points of interests.
DISCLAIMER: The information on this website is not medical science or medical advice. I do not have any medical training aside from my own research and interest in this area. The information I publish is not intended to diagnose, treat, cure or prevent any disease, disorder, pain, injury, deformity, or physical or mental condition. I just report my own results, understanding & research.
![What is Going on in the World? [Summary]](https://pennybutler.com/wp-content/uploads/2023/02/SOUL.jpg)
