00:00 BigBird Tweet 00:03 BigBird & Friends encourage kids to take a covid vaccine to “stay healthy” 00:58 Pfizer Ad tells children taking the vaccine makes them “superheroes” 02:29 If BigBird Told the Truth (someone created a lie-detector video) 03:31 Creepy Microsoft Cartoon aimed at “QR Codes” for Kids 05:28 What it looks like in China when it’s “not a Cartoon” 05:42: CDC Study showing Pfizer Heart Inflammation Reports 05:45 John Stokes Myocarditis – Pfizer 06:10 Ernesto Ramirez – Son Died “enlarged heart” after Pfizer 07:12 Daughter Died – Pfizer 07:21 Children are going into schools without parents consent and getting vaccinated with a trial drug where noone knows the outcome or long-term effects 07:40 NZ Doctors warning of COVID-19 Vaccines in Kids 08:35 Leigh Dundas Human Rights Attorney about removing informed parental consent and turning schools into vaccination centres 09:33 UK – uploaded by Uncle “My niece had her second child last month. She resisted being vaccinated through the pregnancy until a month before the baby was born because she would need a caesarean section and the hospital and doctors told her they would not allow her into the hospital unless she had the jab. Well, you guessed it – she complied and the result is that the baby is back in hospital. Needs a brain scan as they cannot fathom what is causing the jitters which are getting worse. Apparently every test they have done has come back negative and they admit they have no idea what is causing the problem, so they are transferring him to the Great Ormond Street hospital to do further investigations. 09:56 Heart Inflammation – Pfizer 10:16 Roy Butler – 23yo – died from brain bleed after COVID-19 vaccine. 10:19 Speaking on the NSW kids who died from the COVID-19 vaccination rollout at the stadium. 10:53 Clip from Our Voices Matter – Interviews with Australian Victims of the Jab – https://rumble.com/vl731b-victims-of-australia.html 13:11 Friend’s 12yo daughter heart problems after Pfizer 13:45 Julie – Lost her movement and strength in both arms and legs, couldn’t walk, stuttering, seizures and cannot communicate & no hospital knows whats going on. 13:53 USA – Little Sister died from first shot 14:47 – School board hearing “CDC, FDA, Fake News is lying to us about vaccine being safe and effective, urges everyone to speak out and protect the kids. 16:00 Concerned Father stating facts about COVID not effecting kids and they should not get the vaccine. 17:02 Leeds parents outside Costco trying to wake up other parents 17:52 Someone made a cartoon of Fauci being a Snake trying to entice children to get the vaccine out of Mowgli – The Jungle Boy 20:47 Snapshots of Pfizer Kids Myocarditis
Living Document – Updated July 10 2021
My post for staying updated on the latest studies on COVID-19 in relation to Children.
Based on the currently available research, I cannot understand why anyone would think about vaccinating healthy kids with these new vaccines – their risk of getting seriously ill with COVID-19 is extremely small, and spreading from kids to adults remains “exceedingly rare”, and the benefit doesn’t outweigh the short-term “known-risks” and the “completely unknown long-term risks“.
I am a little triggered as I write this because I was just reading all the newest studies to add to the post and found a couple of papers that made my blood boil:
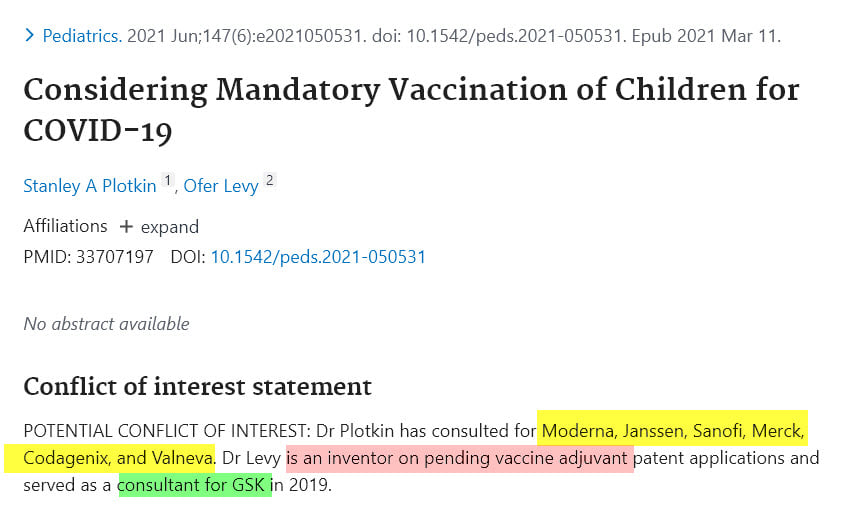
Stanley Plotkin pushing for mandatory vaccination of children(04) Plotkin SA, Levy O. Considering Mandatory Vaccination of Children for COVID-19. Pediatrics. 2021 Jun;147(6):e2021050531. doi: 10.1542/peds.2021-050531. Epub 2021 Mar 11. PMID: 33707197.
and the other calling for mass-testing of children(05) Rubin D, Coffin S. On the Value of COVID-19 Testing for Children Beyond the Spring of 2021. JAMA Netw Open. 2021 Apr 1;4(4):e217850. doi: 10.1001/jamanetworkopen.2021.7850. PMID: 33890994.
Alarmingly, authored by those with connections to Moderna (06)https://www.modernatx.com/, Janssen (07)https://www.janssen.com/us/, Sanofi (08)https://www.sanofi.com/, Merck (09)https://www.merck.com/, Codagenix (10)https://codagenix.com/vaccine-programs/pipeline/, Valneva (11)https://valneva.com/ & GSK (12)https://au.gsk.com/en-au/
And although we don’t choose our names, and this is just a coincidence, and VERY immature that I’m pointing this out.. but I was struck by the name of one of the authors: “Dr. Coffin”. I found it somewhat-fitting considering the extremely obvious conflict of interest. (14) Dr Coffin reported being a member of a data safety monitoring board for Clostridium difficile therapy research done by Merck & Co and serving as an advisor to Genentech about pediatric therapies for COVID.
Dr Plotkin has consulted for Moderna, Janssen, Sanofi, Merck, Codagenix, and Valneva. Dr Levy is an inventor on pending vaccine adjuvant patent applications and served as a consultant for GSK in 2019. (15)Plotkin SA, Levy O. Considering Mandatory Vaccination of Children for COVID-19. Pediatrics. 2021 Jun;147(6):e2021050531. doi: 10.1542/peds.2021-050531. Epub 2021 Mar 11. PMID: 33707197. Dr Coffin reported being a member of a data safety monitoring board for Clostridium difficile therapy research done by Merck & Co and serving as an advisor to Genentech about pediatric therapies for COVID. (16) Rubin D, Coffin S. On the Value of COVID-19 Testing for Children Beyond the Spring of 2021. JAMA Netw Open. 2021 Apr 1;4(4):e217850. doi: 10.1001/jamanetworkopen.2021.7850. PMID: 33890994.
#PleaseExplain
Keypoints to address & get out of the way…
“But what about India?” and “I heard Indonesian kids are dying!”
Comparing poverty-stricken areas to the rest of the world is not comparing apples with apples, and we should be extremely mindful of headlines that create irrational fear that our own children face the same level of danger or trying to coerce children into taking an experimental vaccine to “protect grandma” when the studies show that the spread from children to adults “globally” is negligible.
Interventions aimed at children are expected to have a small impact on reducing SARS-CoV-2 transmission.” – Clinical Infectious Diseases, March 2021 (24)Antoni Soriano-Arandes, PhD, Anna Gatell, MD, Pepe Serrano, MD, Mireia Biosca, PhD, Ferran Campillo, MD, Ramon Capdevila, MD, Anna Fàbrega, MD, Zulema Lobato, MD, Núria López, MD/MSc, Ana Mª Moreno, MD, Miriam Poblet, MD, Maria Teresa … Click for full citation
USA, UK, Italy, Germany, Spain, France, South Korea – deaths from COVID-19 in children remain rare up to February 2021, at 0.19 per 100 000 population, comprising 0.54% of the estimated total mortality from all causes in a normal year.” (25)Children and young people remain at low risk of COVID-19 mortality – Bhopal, The Lancet Child and Adolescent Health, March 2021
Germany – “Our investigation suggests that child-to-child transmission in schools and childcare facilities is uncommon and not the primary cause of SARS-CoV-2 infection in children.” (29)Germany -Citation style for this article: Ehrhardt J, Ekinci A, Krehl H, Meincke M, Finci I, Klein J, Geisel B, Wagner-Wiening C, Eichner M, Brockmann SO. Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools … Click for full citation
Several on-going studies (Netherlands) “Researching the role of children in the spread of the virus” updated every Tuesday.(37) (Netherlands) “Researching the role of children in the spread of the virus” updated every Tuesday.
Downloads
The risk v benefit calculation does NOT support administering experimental Covid-19 vaccines to healthy children…
COVID-19 vaccination in children – major ethical concerns | PDF(38)COVID-19 vaccination in children – major ethical concerns – March 17, 2021 – Dr Ros Jones – Retired Consultant Paediatrician
Covid policies and harms to children | PDF(39)Covid policies and harms to children – March 17, 2021 – Dr Ros Jones (Retired Consultant Paediatrician) & Dr Zenobia Storah (Child and Adolescent Clinical Psychologist)
Education Minister on Mass-Testing in Schools | PDF(40)Education Minister on Mass-Testing in Schools | PDF
Headteachers and Teachers re Covid-19 Vaccination of Children in Schools | PDF(41)Headteachers and Teachers re Covid-19 Vaccination of Children in Schools | PDF
Urgent re Emergency Authorisation of the Pfizer Covid-19 vaccine for Children | PDF(42)Urgent re Emergency Authorisation of the Pfizer Covid-19 vaccine for Children | PDF Grave concerns about this emergency authorisation, citing evidence of known and potential harms to children that may result and the serious ethical issues this decision raises. Given that these vaccines will have virtually no benefit to the children themselves, it is profoundly unethical and indefensible to vaccinate children, especially with an experimental vaccine using novel technology, in what appears to be a misguided attempt to protect adults and achieve herd immunity. We call on the MHRA to exercise caution and immediately reverse their decision.
Regarding Covid-19 Vaccination of Children | PDF(43)Regarding Covid-19 Vaccination of Children | PDF This open letter to child health experts and regulators raises serious concerns about the administration of Covid-19 vaccines into healthy children. We reference current scientific evidence that clearly shows the ‘risk v benefit’ calculation does NOT support administering experimental Covid-19 vaccines to healthy children, who have no risk from Covid-19, yet face known and unknown risks from the vaccines.
Senator LAMBIE: I realise it’s only early days with the vaccine. We’ve obviously got pregnant women out there. What is the advice that cabinet or whatever is coming up with to vaccinate these women who are carrying babies? Are there any terms that they should be vaccinating them—at one month, two months or three months?
Dr Murphy : The ATAGI advice is that, at the moment, there’s no evidence that any of the vaccines have any adverse impact on pregnancy. There has been quite a bit of vaccination of people who turned out to be pregnant in the UK—people who didn’t know they were pregnant—and there’s been no evidence of what we call teratogenic or other adverse effects of the vaccine. But, in the absence of any specific studies in pregnant women, the advice has been that, at this stage, people should have a discussion with their doctor. I might ask Professor Skerritt to comment because he has the actual specific advice there, presumably, from the TGA.
Dr Skerritt : The specific advice from the TGA is that the safety and efficacy of the vaccine wasn’t assessed during clinical trials in pregnant women. However, people—for example, a nurse who may be working in an infectious diseases department or an emergency department—can choose and elect in consultation with their doctor to be vaccinated. There’s a very recent study that has been looked at in the US where they actually have looked at several hundred pregnancies and found no evidence of any birth defects or adverse outcomes on the pregnancy. We’re hoping that it will be published in the next couple of weeks. So, through the regulators’ grapevine, there’s a positive study—that was mainly with the Pfizer vaccine and the Moderna vaccine—showing that there are no adverse effects of the vaccination during pregnancy, and that’s really good news.
Dr Murphy : There are resources on our website, Senator Lambie, for any pregnant woman who seeks information, and for providers who want to look at the issue there’s significant information.
Senator LAMBIE: If that causes any defects or any issues when the baby is born, will they be covered with any sort of compensation?
Dr Murphy : There is, again, no evidence that that might be the case, but obviously—
Senator LAMBIE: That’s not what I asked you, Mr Murphy. I asked you: are they covered by a compensation system or scheme?
Dr Murphy : Obviously, if there were proven adverse effects from a vaccine, whether it was a birth defect or any other effect, there would be well-established avenues for getting compensation via our legal system, and, as you know, the Commonwealth has provided certain indemnities to the vaccine manufacturers to protect against that. So, yes, there are existing mechanisms if such a thing is proven, but there is no evidence that it’s the case.
Senator LAMBIE: I want to talk about children. We know that children can catch COVID-19—that’s now swinging back around—and that there are trials, but do we know if the vaccines are safe for young children? And to be protected will they need a vaccine?
Dr Murphy : I might get Professor Kelly to talk to that. There are trials being done at the moment in teenagers, who seem more commonly to get clinically evident COVID than younger children do. But the main reason to want to vaccinate children would be to create herd immunity. Very, very few children have clinically apparent COVID disease, and the very young children—primary school children—often don’t get the virus at all. It doesn’t seem to transmit very well. It does seem to transmit in older children, secondary-school-age children, and for that reason there are trials underway to make sure the vaccines are safe and effective. If they are safe and effective, we would probably, like most countries, want to embark on a program of vaccinating older children to create greater herd immunity to stop transmission. Professor Kelly might want to address that.
Prof. Kelly : I think it’s a very important component. Thank you for the question, Senator. For the reasons that Professor Murphy has mentioned, it’s not so much to protect the children, because we’ve found right around the world that that hasn’t been a major issue in terms of COVID—surprisingly; it’s very unusual for a respiratory infection like this to affect adults more than children, but that appears to be the case. It will be an important component of our vaccine rollout eventually. At the moment, there are trials, I believe—and Professor Skerritt will of course know more about these through his contacts internationally—down to the age of five—
Dr Skerritt : Five or six.
Prof. Kelly : five or six—for several of the vaccine candidates. So we look forward to those matters, but, at the moment, the TGA has approved only 18 and over for the AstraZeneca vaccine and 16 and over for the Pfizer vaccine, on the basis of the trial data that they’ve been presented with.
Dr Skerritt : But there is an expectation, in talking with some of the companies—and I’ve got to watch what I say because it’s commercial-in-confidence. Some of the companies that are already providing vaccines in Australia are expecting to submit regulatory data on children and adolescents later this year. That will give the Commonwealth the ability to decide whether or not to lower the age threshold. This is very common, for example, with the flu vaccines. The trials and data are originally generated in adults, and then later on adolescents and children are added to those trials.
Dr Murphy : There’s an important difference between flu and COVID, in that flu can be a very nasty disease in young children—
Dr Skerritt : For young children, yes.
Dr Murphy : and COVID is not a nasty disease in young children.
Dr Skerritt : But the general thing is that the very first trials you do with any vaccine are with healthy adults. For ethics reasons, they don’t round up a bunch of schoolkids to do those trials; they start with healthy adults over 18. As Professor Murphy said, flu is worse for children than COVID appears to be, as far as the symptoms.
Senator LAMBIE: Are you in discussions behind closed doors about getting herd immunity in our population if children aren’t vaccinated? Those under five or six. Is there any discussion on vaccinating them to get that herd immunity going?
Prof. Kelly : I might answer that. The issue of herd immunity is an important one to consider. It’s not an all or none phenomenon. The more people that are vaccinated, the more protection we have as a community. As you know, Senator, the vaccine rollout plan is based very much on vaccinating the vulnerable communities first and then working through the wider community. It’s true that the proportion of the Australian community who are at a younger age, who currently can’t be vaccinated and haven’t, in general, been exposed to the virus, could be a pool to recreate outbreaks in Australia, even if we’ve got a very high rate of vaccination within the adult community. So that is a matter; it’s a balancing act, again. Of course, we’re not going to start any vaccination program in children until we have that go-ahead from the TGA that it’s safe.
Senator LAMBIE: The question is: does anybody know whether we will be able to get herd immunity in our population if children are not vaccinated? Do we know that yet?
Prof. Kelly : We could, but it would require a very high rate of vaccination in adults. We need to get over 70 per cent to get herd immunity, and the higher, the better. With about 30 per cent of the population under the age of 18 in Australia, that would be difficult.
CHAIR: Would you need almost 100 per cent of the adult population to get to herd immunity without children?
Prof. Kelly : Correct.
Senator LAMBIE: The Pfizer and the AstraZeneca are approved for people over different ages: 16 for Pfizer and 18 for the AstraZeneca.
Senator LAMBIE: Are there any early results on whether certain vaccines are safer for children under the age of 10, five, or however you’d break it up? Is AstraZeneca less safe for children than the mRNA vaccines?
Dr Skerritt : Those studies, those trials, are still underway globally. Some of them have completed recruiting children and they’ve now vaccinated all of those kids. They’re waiting, obviously for a few months, to see whether there are differences in the vaccinated group of children versus the unvaccinated group of children or adolescents. As I indicated earlier, those trials will read out—we’ll get the results later in the year. There’s no evidence, for example, that one particular vaccine is more or less safe or effective in children than another vaccine. But, as more companies and clinical research groups are involved in those trials, we’ll be able to see the data, for example, for maybe three or even four vaccines by the end of the year.
Senator LAMBIE: Do children need to be vaccinated before we can open the borders and go back to living life more normally, or are we’re going to leave them out and just see what happens?
Prof. Kelly : As I mentioned in a previous answer, Senator, that is, in fact, the information that’s been sought and the advice that has been sought from the Australian Health Protection Principal Committee to the national cabinet—to decide about border and other opening matters. That’s work that’s currently underway.
CHAIR: So the level of vaccine deployment or the level of vaccination across the community will be a key component of that advice?
Prof. Kelly : I think it’s the absolutely most key part.
Senator LAMBIE: Have we got as far as asking if we have enough of the right vaccines to vaccinate our kids when it’s safe to do so? Do we have plans ready for a vaccine rollout for the kids? How would it work; or are we not that far yet?
Dr Murphy : Obviously we wouldn’t be using the AstraZeneca vaccine as a preference now for people under 50. But we have 40 million doses of the Pfizer vaccine coming, and eventually over 50 million doses of the Novavax vaccine coming later in the year. So we have plenty. There’s no suggestion that Novavax would have any age restrictions to it. We have plenty of vaccines on order to cover all of the Australian population twice over.
Senator LAMBIE: Have we got as far as the vaccine rollout for the kids? How would that work?
Dr Murphy : I think it’s a bit speculative at the moment until we have the evidence of safety and efficacy. But, in general, vaccine rollout to children is done through school based programs. They are the most effective way to get mass vaccination of children. The states and territories have a primary role in school based programs and are very experienced at them, and they’re very successful programs. So, if we got to that, that’s likely how we would do it, obviously supplementing it with general practitioners. It depends on the age range you’re talking about. If we eventually got down to quite young children, you might use other avenues. But, in the main, school based programs are the preferred option.
Ms Edwards : I can add that, in the vaccine rollout strategy since it was first announced in January, phase 3 has always envisaged the vaccination of children if and when a product is approved for that age. The age was recently reduced to under 16, subject to a new product, because the Pfizer vaccine is actually approved for people of 16 and above, and we have indicated that we would consider school based programs. But, of course, in regard to the logistics of what sort of vaccine it is and how it might be done, I’d expect we’d potentially be using all of the available mechanisms of vaccination for children, assuming that the product that’s approved for them in due course can be delivered through those mechanisms. So, yes, we have given some thought to it, but exactly how it would happen would depend on what happens in the meantime with an authorised product.
I’m also currently drafting another post with all the Questionable Conflicts of Interest 👀 and all the ties that is breaking my heart and breaking whatever trust I had left with these organizations & governments. Despite what we may be led to believe, there is not a lot of transparency going on surrounding these vaccines.
(I need a break from that other post because it’s giving me heart-palpitations) but I intend to publish it in the next couple of days. I will try and remember to update this post with the link, but if I forget, it will definitely be listed on both the COVID summary page and in the GovTalk category when published.
Vaccinating Kids has already begun in the UK:
Open Letter from the UK Medical Freedom Alliance (46)UK Medical Freedom Alliance Re: Safety and Ethical Concerns of using Covid-19 Vaccines in Healthy Children
The argument that vaccinating children will accelerate herd immunity lacks any scientific basis. Herd immunity was developed as an epidemiological and not an immunological concept, relating to immunity that is acquired naturally. There are currently no data to show that the current Covid-19 vaccines prevent infection with, or transmission of, the virus. Hence vaccination only benefits the recipient. It is also not known how long vaccine-induced immunity will last, but it is widely expected to require booster doses at least once a year. Hence, focussing on vaccine-induced antibodies as the sole or even main mode of developing herd immunity appears to disregard immunological science. (55)https://childrenshealthdefense.org/defender/herd-immunity-myth-covid-vaccines-kids-deceptive-dangerous/(56)https://pubmed.ncbi.nlm.nih.gov/32908300/(57)https://www.bmj.com/content/370/bmj.m3563
We argue that for children, vaccine-induced antibody-dependent immunity to SARS-CoV-2 is inferior to natural immunity, as it does not cover the full spectrum of protective immunity (mucosal immunity, IgA, and T-cell immunity to the whole virus) and may be only short-lived. Naturally acquired immunity, which is completely safe for children to obtain, is expected by scientists to be long-lasting (58)https://www.nature.com/articles/s41586-021-03207-w as it has been from SARS-CoV-1, where those infected have been found to retain memory T-cell immunity 17 years post-infection. (59)https://pubmed.ncbi.nlm.nih.gov/32668444/ Natural immunity is therefore likely to be a better strategy for children, avoiding the need for multiple, recurrent vaccine booster doses over a lifetime. For the wider population and public health, it may be detrimental to roll out the vaccines to groups who are not at risk from SARS-CoV-2, and preferable to allow significant population immunity to develop naturally, by leaving negligible risk groups, such as children, unvaccinated. There is compelling research suggesting that imperfect, non-sterilising, vaccines can promote the evolution of pathogen virulence of mutations, which would prolong the pandemic. (60)https://www.nature.com/articles/414751a. This concern has recently been raised relating to Covid-19 vaccines (61)https://www.wbur.org/npr/965940914/covid-19-vaccines-could-add-fuel-to-evolution-of-more-coronavirus-mutationsPotential.
Potential Risks to Children from Experimental Covid-19 Vaccines
Experimental Vaccines with Novel technologies
All Phase 3 Covid-19 vaccine trials are ongoing and not due to conclude until late 2022/early 2023. The vaccines are, therefore, currently experimental with only limited short-term and no long-term safety data available. In addition, many are using a completely new mRNA vaccine technology, which has never previously been approved for use in humans. (62)https://www.immunology.org/coronavirus/connect-coronavirus-public-engagement-resources/types-vaccines-for-covid-19 Some are using a different technology – viral vector DNA vaccines – that has only had limited use before in Ebola vaccines.
The UK Government have already granted immunity from liability for harms to all Covid-19 vaccine manufacturers which they demanded. An Astra Zeneca spokesperson said that “this is a unique situation where we as a company simply cannot take the risk if in … four years the vaccine is showing side effects” (68)https://www.reuters.com/article/us-astrazeneca-results-vaccine-liability-idUSKCN24V2EN. If this risk is significant enough for the manufacturers to anticipate economic loss, children should not be expected to take the same risk, jeopardising their long-term health.
PubMed is a search engine that accesses the database on all science & biomedical topics. (80)About PubMed https://pubmed.ncbi.nlm.nih.gov/about/ (Ensure you always double-check the conflict of interests section to discern / weigh-up potential biases, read through the data to see if they are not skewing the conclusion in favour of their personal bias, and look for any ‘discussion’ on the particular paper to see if other researchers are disputing the research or pointing out discrepancies in their data.)
There are over 5,500 results in PubMed for the search terms “children” and “covid-19” in the title/abstract.
There are over 1,800 results in PubMed for the search terms (children[Title]) AND (covid-19[Title]) – almost 1,000 of them were published this year (2021).
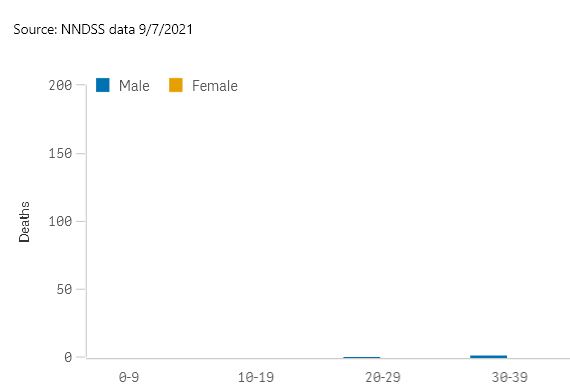
Tell me again why we’re vaccinating our kids? No Covid deaths in 0-19-year-olds in Australia since the pandemic began & children have a survival rate of 99.999%. pic.twitter.com/SA36xR9Nf4
Australian research shows why children do not need to receive Covid vaccines – they have innate immunity. Vaccines for other childhood diseases – yes. Covid – no. https://t.co/bPgSZy9nih… pic.twitter.com/Nc4mR1jqv3
160 Year 12 students at St Joseph’s College have been given the Pfizer vaccine, even though the program has only officially been rolled out to people aged 40 and above. How can teens, many of whom would not be 18, give informed consent? Is this even legal? https://t.co/ih4R3D24Ar
COVID and schools: the evidence for reopening safely After a school term filled with anxiety and vitriol, researchers assess the spread of coronavirus and the prospects for a return to normal.https://t.co/nkHzlMjgUW
When the media won’t hold the government accountable for the harm and deaths their COVID-19 policies are responsible for, the AVN will! #KeepingTheBastardsHonest since 1994https://t.co/mNfV3Obbb4
Here is a fun game. Can anyone else spot the logic and data analysis flaws in this “Nature” analysis? To both Jill and I, they are immediately obvious. Maybe a red pill is required. To us, this looks like overt propaganda.https://t.co/1ZJFvemuOg
Plotkin SA, Levy O. Considering Mandatory Vaccination of Children for COVID-19. Pediatrics. 2021 Jun;147(6):e2021050531. doi: 10.1542/peds.2021-050531. Epub 2021 Mar 11. PMID: 33707197.
Rubin D, Coffin S. On the Value of COVID-19 Testing for Children Beyond the Spring of 2021. JAMA Netw Open. 2021 Apr 1;4(4):e217850. doi: 10.1001/jamanetworkopen.2021.7850. PMID: 33890994.
Dr Coffin reported being a member of a data safety monitoring board for Clostridium difficile therapy research done by Merck & Co and serving as an advisor to Genentech about pediatric therapies for COVID.
Plotkin SA, Levy O. Considering Mandatory Vaccination of Children for COVID-19. Pediatrics. 2021 Jun;147(6):e2021050531. doi: 10.1542/peds.2021-050531. Epub 2021 Mar 11. PMID: 33707197.
Boast A, Munro A, Goldstein H. An evidence summary of Paediatric COVID-19 literature, Don’t Forget the Bubbles, 2020. Available at: https://doi.org/10.31440/DFTB.24063
Covid policies and harms to children – March 17, 2021 – Dr Ros Jones (Retired Consultant Paediatrician) & Dr Zenobia Storah (Child and Adolescent Clinical Psychologist)
Truth-seeker, ever-questioning, ever-learning, ever-researching, ever delving further and deeper, ever trying to 'figure it out'. This site is a legacy of sorts, a place to collect thoughts, notes, book summaries, & random points of interests.
DISCLAIMER: The information on this website is not medical science or medical advice. I do not have any medical training aside from my own research and interest in this area. The information I publish is not intended to diagnose, treat, cure or prevent any disease, disorder, pain, injury, deformity, or physical or mental condition. I just report my own results, understanding & research.




 Aussies
Aussies 
![Covid-19 and the Global Predators – We are the Prey [Dr Peter Breggin]](https://pennybutler.com/wp-content/uploads/2022/10/DrPeterBreggin-GlobalPredators.jpg)