PCR-Test Videos & Links
- Updated:11 months ago
- Reading Time:60Minutes
- Post Words:15849Words

Just wanted to collect all interesting PCR-Test related videos & studies on one page. See all my posts tagged PCR.
Living Document. Started 2 July 2021. Last updated 17 October 2022
Quick Explainer: 2 Minute Video giving rundown on PCR-Tests (01) 2 Minute 101 on PCR-Tests
PCR tests cannot determine an acute infection, ongoing infectiousness, and actual disease, especially if ct values are not taken into account. – The Trouble With PCR Tests – Swiss Policy Research (02)The Trouble With PCR Tests – Swiss Policy Research
A French Study (June, 2021) has shown that when the PCR test is run at 25 cycles, about 70% of samples were genuinely positive (infectious).
However, when the test is run at a threshold of 30 cycles, only 20% of samples were infectious.
At 35 cycles, only 3% of samples were infectious.
And when run above 35 cycles – Zero samples were infectious.. (03)Rita Jaafar, Sarah Aherfi, Nathalie Wurtz, Clio Grimaldier, Thuan Van Hoang, Philippe Colson, Didier Raoult, Bernard La Scola, Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including … Click for full citation
A USA Cross-Country Analysis (April 2021) has shown that national PCR testing rates have had no influence at all on covid mortality. (04)A Cross-Country Analysis of the Determinants of COVID-19 Fatalities – 23 Apr 21
A German study (June 2021) re-analyzed PCR tests of 160,000 people and concluded “In light of our findings that more than half of individuals with positive PCR test results are unlikely to have been infectious”. (05)Stang A, Robers J, Schonert B, Jöckel KH, Spelsberg A, Keil U, Cullen P. The performance of the SARS-CoV-2 RT-PCR test as a tool for detecting SARS-CoV-2 infection in the population. J Infect. 2021 Jun 1:S0163-4453(21)00265-6. doi: … Click for full citation
The FDA issued a Press Release (May 19, 2021) FDA Advises Against Use of SARS-CoV-2 Antibody Test Results to Evaluate Immunity or Protection From COVID-19, Including After Vaccination (06)FDA document, May 19, 2021: FDA Advises Against Use of SARS-CoV-2 Antibody Test Results to Evaluate Immunity or Protection From COVID-19, Including After Vaccination – FDA Press Release
Kevin McKernan – R&D lead Human Genome Project at MIT/WIBR – publishes PCR-related ‘explainers’ criticizing how the PCR-test is being used during this ‘Pandemic’:
The Live-Dead qRT-PCR problem, the testing industrial complex and its impact on society. (07)Archive.org backup of Live-Dead qRT-PCR problem Thread by Kevin McKernan
We are now ruled by qPCR right and the transparency on the process is shameful. Kevin’s explainers: (08)The Live-Dead qRT-PCR problem (09)Threadreader: Kevin McKernan – R&D lead Human Genome Project at MIT/WIBR (10)Follow Kevin on Twitter (11)Threadreader: Kevin McKernan: But but… you ran it to 40-45 cycles? (12)Threadreader: Kevin McKernan: “Zero evidence of asymptomatic spread. (13)Threadreader: Kevin McKernan: Cliff Notes of 4 papers that Dissolve the Corman-Drosten RT-qPCR test. (14)Threadreader: Kevin McKernan: It’s frightening that no one seems to care about the Nuremberg code. Let’s walk through how many of these tenets are violated each day with qPCR testing of asymptomatic people and quarantining them on the results of … Click for full citation (15)Threadreader: Kevin McKernan: Now that we’ve gone over Nuremberg….Lets have a look at the published massive scale psychological experiment Facebook performed on its customers. (16)Threadreader: Kevin McKernan: This is the Final nail in the coffin of the current qPCR testing strategy. (17)Threadreader: Kevin McKernan: We have written another 60 page dissection of the Drosten PCR protocol. This should end all of the criticism of the initial retraction request not having enough “wet-lab” proof. 20 peer reviewed papers showing … Click for full citation
The New York Times (Aug 2020) did an extensive piece investigating various labs and PCR-Test Protocols throughout the USA. Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. (18)NY Times: Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.
“I’m shocked that people would think that 40 could represent a positive,” she said. Julia Morrison, a virologist at the University of California. “A more reasonable cutoff would be 30 to 35“.
Harvard epidemiologist, Dr. Michael Mina: “upwards of 90% of positive tests in Massachusetts with a 40 Ct threshold would have been negative at 30 Ct”
Many US labs work with 35 to 45 cycles, (19)NY Times 35-45 Cycles while many European labs work with 30 to 40 cycles. (20)European Labs 30-40 Cycles
Response to NY Times article from the perspective of a hospital COVID testing laboratory (Source: Yale) saying they “need to do it” “just in case” (21)Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. – NY Times Expose 29 Aug 2020 – PDF Summary
The CDC (Dec 2020) was still recommending 40 cycles. (22)CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel – FDA/CDC PDF
A UK study (Dec 2020) published in the British Medical Journal found that 58% of positive tests at the University of Birmingham were false positives. (23)Armstrong S. Covid-19: Tests on students are highly inaccurate, early findings show BMJ 2020; 371 :m4941 doi:10.1136/bmj.m4941
COVID-19 positive cases down 62% since World Health Organization updated PCR guidance – Feb 21, 2021
A Canadian study (May 2020) reported no positive viral cultures with a Ct > 24. (24)Jared Bullard, Kerry Dust, Duane Funk, James E Strong, David Alexander, Lauren Garnett, Carl Boodman, Alexander Bello, Adam Hedley, Zachary Schiffman, Kaylie Doan, Nathalie Bastien, Yan Li, Paul G Van Caeseele, Guillaume Poliquin, Predicting … Click for full citation
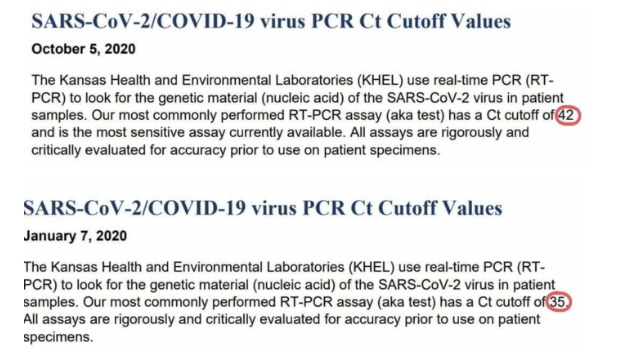
The Kansas Department of Health and Environment’s Health and Environmental Laboratories (Jan 2021) reduced (25)Screengrab of PCR recommendations changing from 42 to 35 – KDHE quietly reduced cycle threshold on COVID tests – Jan 21, 2021 the cycle threshold for its real-time COVID-19 test from 42 to 35 cycles.
KHEL (Oct, 2020) said their most commonly-used test “has a Ct cutoff of 42 and is the most sensitive assay [test] currently available.” (expand screengrab below)
KHEL (Jan 7, 2021), reduced the Ct cutoff to 35, and the last half of that sentence omitted.(26) SARS-CoV-2/COVID-19 virus PCR Ct Cutoff Values – Kansas Dept Health
“Cycle thresholds between 12 and 36 are considered positive;
results between 36 and 40 cycles are considered marginally positive,
and anything over 40 cycles is considered negative.”
– Bioningentech Manual (one of the manufacturers of the COVID PCR-Tests)
Corman-Drosten Review Report – Curated By An International Consortium Of Scientists In Life Sciences (Icsls) (Nov 2020 – Jan 2021)
External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results. (27)Corman-Drosten Review Report
Swiss Policy Research keeps updating their The failure of PCR mass testing page with the latest studies. (28)The failure of PCR mass testing – Swiss Policy Research
“PCR Tests are useless at detecting COVID-19 … but very good at keeping us under house-arrest”
Dr. Vernon Coleman
PCR-Tests are the centrepiece to this entire pandemic. Not only do we keep going into ‘lockdown’ and have our movements tracked because of PCR-Testing, but all the ‘case-counts & death-counts’ depend on these tests. New powers have been given to governments and other companies, our economy is ruined, emergency laws enacted, rights-surrended, jobs-lost, elderly dying alone, kids in masks, billions of tax-payer funded federal government spending, needing to go into quarantine – even if you are not infectious, and most importantly: the experimental vaccine efficiency data was “approved” because of these tests – EVERYTHING – Every part of this WHOLE pandemic centres around this PCR-Test.
It is known by everyone – governments, media, virologists, labs, scientists, doctors, the World Health Organization, the CDC, the FDA, lawyers, and even talked about on mainstream media, and so most of the general public would know that they are unreliable as well – and yet it’s significance in producing false-results – it’s inaccuracy – and it’s use on asymptomatic people is insanity and only serves in a way to produce fear-mongering headlines, which cause the people to demand their own lockdowns, and cause a division of discrimination and finger-pointing amongst the population, and used by governments to promote ‘vax the nation’ campaigns, and the forced-vaccination of these experimental still-in-trial vaccines to our front-line workers – is being downplayed or dismissed. Billions have been invested because of the results of these tests. Dedicated Quarantine Centres are being built, Laboratories being built, Laws are being changed. Why?
2022
PCR based on computer-modelled virus
13 July 2022 Rumble | Telegram Dr Kevin P. Corbett – Nurse & Health Scientist
“… there’s something about the existence of the virus that the official scientists and some of the distant scientists don’t want to go near, which is due to with the fact that the initial test – the PCR test methodology – was based on a computer modelled virus.
It was not based on a purified isolate from real patients – because China didn’t have that when they gave the data to the Corman Drosten authors to “model the virus”. They didn’t have a sequence that was developed from a pure isolate:
So they hadn’t taken blood from patients and isolated “from” that, a pariticular virus. They had some elements of a genetic code, which they modelled in silico computer modelling, to produce what they said was a complete sequence.
And that was the basis for the PCR test that is now being used.
They admitted that they developed the test based on in silico modelled genetic sequence – not a real element taken from patients.
That’s true. That’s not a conspiracy theory. That’s the truth.
And the W.H.O. in its own document, given to the NHS, and I got a copy of it from Maria Zambon herself, it said on one of the pages, diagnosis for SARS-CoV-2 should not be based on isolation of the virus. So it’s telling the governments of the world, don’t bother isolating it, “Trust us—it’s there”.
People will say that I’m speaking rubbish, and I’ll be castigated. I don’t care. That is the truth. A virus that has never been purified, a disease that is based on a set of generic symptoms that could be anything,”
https://web.archive.org/web/20210418081038/https://covileaks.co.uk/
2021
November 25, 2021
PCR Testing | Planet Lockdown Film (29)PCR Testing | Planet Lockdown Film
Wolfgang Wodarg (Doctor, FMR, Public Health Official, Former Member German Parliament):
In January 2020, another thing started, and that was there was a test, a PCR test that was invented by Mr Droston, and it was accepted by WHO, and WHO said if the test is positive, we have a “case” of Covid-19.
Alexandra Henrion-Caude (Geneticist, France):
I realized very quickly that it was used to define “cases”.
“Cases” for us, in our language, is about “patients”.
And here, the “cases’ became the positivity to PCR.
So forget about the individual, it was just a result from a technique.
Knut Wittkowski (Epidemiologist, New York City):
So the meaning of the word “case” has been changed during the data collection of an epidemic, and that is – for an epidemiologist and for everybody else – the worst thing that can happen.
They’re now calling apples, oranges. And now there are many “oranges” – many more than there were before.
Wolfgang Wodarg (Doctor, FMR, Public Health Official, Former Member German Parliament):
And this is how they started counting the “cases”.
What they counted, was the activity of “testing”, and the more they tested, the more “cases” they found.
Knut Wittkowski (Epidemiologist, New York City):
It creates fear.
It creates an impression that something ‘bad’ is happening, because there are so many “cases”.
No – there are not so many cases.
Claus Kohnlein (Internal Medicine Doctor, Kiel, Author “Virus Mania”)
What we experiencing is nothing more than a PCR Test pandemic.
Knut Wittkowski (Epidemiologist, New York City):
It is so absurd. We have created a situation where so many people are so fearful that reality doesn’t enter their mind anymore.
Alexandra Henrion-Caude (Geneticist, France):
We have finally built this crisis with this new definition of cases, based on this PCR testing.
Reiner Fuellmich (Global Fraud Attorney)
Even the World Health Organization agrees that it’s not enough for you to test positive on a PCR test – you need “symptoms”. And it’s never in the history of mankind, in the history of medicine, there has never been testing of “healthy people”.
Scott Jensen (Doctor, State Senator, MN)
The guy who discovered PCR techniques – he died in August, 2019 – said this is not a technology to be used for diagnosing viral disease. This is a technology that can help us take a small strand of DNA material, and if you will, manufacture billions times more, so we work with it and ‘learn’.
Sucharit Bhakdi (Biologist, Immunologist)
The PCR method, developed by Mullis who got the Nobel prize for this – he himself said “Do not use this test for diagnosis”. (30)Kary Mullis on the PCR: https://www.youtube.com/watch?v=iWOJKuSKw5c
You should not be using this test on people without symptoms.
Michael Yeadon (Former Pfizer VP)
Mass-testing without symptoms has no underpinning science at all. It’s just a way of frightening people. You should disregard all announcements of “case rates” in your community, because they’re completely fraudulent.
Wolfgang Wodarg (Doctor, FMR, Public Health Official, Former Member German Parliament):
The test is positive with viruses that existed long-ago, that existed before. They are positive with all better coronaviruses, with lots of SARS viruses, that exist around 20 years already, all over the world.
So, the one who made the test knew exactly that this test would give many positive results.
Sucharit Bhakdi (Biologist, Immunologist)
This test should be trashed immediately. Worldwide. And it should be considered a criminal act for anyone to be sent to quarantine, because this test was positive.
Dr. Sam Bailey PCR Videos (Click Title to Open)
PCR: The Good, The Bad and The Bustin – OCT 2021 (31)PCR: The Good, The Bad and The Bustin – OCT 2021
- Stephen Andrew Bustin (32)Stephen Andrew Bustin: https://www.researchgate.net/profile/Stephen-Bustin
- The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments (33)The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments: https://www.gene-quantification.de/miqe-bustin-et-al-clin-chem-2009.pdf
- RT-qPCR—Facts and Fallacies: An Interview With Professor Stephen Bustin (34)RT-qPCR—Facts and Fallacies: An Interview With Professor Stephen Bustin: https://www.technologynetworks.com/diagnostics/articles/rt-qpcrfacts-and-fallacies-an-interview-with-professor-stephen-bustin-346520
- WHO Director-General’s opening remarks at the media briefing on COVID-19 – 16 March 2020 (35)WHO Director-General’s opening remarks at the media briefing on COVID-19 – 16 March 2020: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—16-march-2020
- Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19 (36)Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19: https://onlinelibrary.wiley.com/doi/10.1002/jmv.25786
- Planet Waves FM Interview with Dr. Stephen Bustin – February 10, 2021 (37)Planet Waves FM Interview with Dr. Stephen Bustin – February 10, 2021: https://planetwaves.net/planet-waves-fm-interview-with-dr-stephen-bustin/
- COVID-19 and Diagnostic Testing for SARS-CoV-2 by RT-qPCR—Facts and Fallacies (38)COVID-19 and Diagnostic Testing for SARS-CoV-2 by RT-qPCR—Facts and Fallacies: https://arro.anglia.ac.uk/id/eprint/706392/6/Bustin_et_al_2021.pdf
- Portuguese Court Rules PCR Tests “Unreliable” & Quarantines “Unlawful” (39)Portuguese Court Rules PCR Tests “Unreliable” & Quarantines “Unlawful”: https://off-guardian.org/2020/11/20/portuguese-court-rules-pcr-tests-unreliable-quarantines-unlawful/
- Austrian court overturns judgment: PCR test not suitable for diagnosis (40)Austrian court overturns judgment: PCR test not suitable for diagnosis: https://mainland.press/2021/04/02/austrian-court-overturns-judgment-pcr-test-not-suitable-for-diagnosis/
- Austrian court ruling on the PCR (German) (41)Austrian court ruling on the PCR (German): https://wp.tagesstimme.com/wp-content/uploads/2021/03/Verwaltungsgericht_FPOe-Versammlung.pdf
- Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction–Based SARS-CoV-2 Tests by Time Since Exposure (42)Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction–Based SARS-CoV-2 Tests by Time Since Exposure: https://www.acpjournals.org/doi/10.7326/M20-1495
The PCR Hustle – SEPT 2021 (43)The PCR Hustle – SEPT 2021
- Counties Manukau- What happens to your Covid-19 Test? (44)Counties Manukau- What happens to your Covid-19 Test? https://www.countiesmanukau.health.nz/news/curious-about-what-happens-to-your-covid-19-test/
- Kary Mullis on the PCR (45)Kary Mullis on the PCR: https://www.youtube.com/watch?v=iWOJKuSKw5c
- Celia Farber ft. David Crowe, 7 April, 2020 (46)Celia Farber ft. David Crowe, 7 April, 2020 https://uncoverdc.com/2020/04/07/was-the-covid-19-test-meant-to-detect-a-virus/
- NZ Ministry of Health OIA request PCR test costs – Ref. H202007128
- Australian Covid Medical Network (47)Australian Covid Medical Network: https://www.covidmedicalnetwork.com/open-letters/first-do-no-harm.aspx
- NZ’s Covid Leaderboard (48)NZ’s Covid Leaderboard: https://www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-19-data-and-statistics/covid-19-current-cases
- University of Otago – Coronavirus testing – how does it work? (49)University of Otago – Coronavirus testing – how does it work?: https://www.otago.ac.nz/biochemistry/research/otago736925.html
- Otago Biochemistry -How does RT-PCR work? (50)Otago Biochemistry -How does RT-PCR work?: https://www.youtube.com/watch?v=MU8-zIZagBc
- The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments (51)The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments: https://www.gene-quantification.de/miqe-bustin-et-al-clin-chem-2009.pdf
- Planet Waves FM Interview with Stephen Bustin, conducted by Eric F. Coppolino (MP3) (52)Planet Waves FM Interview with Stephen Bustin, conducted by Eric F. Coppolino: http://chironreturn.org/audio/210201-steve-bustin.mp3
Once Upon A Time in Wuhan…. – JUL 2021 (53)Once Upon A Time in Wuhan…. – JUL 2021
- Dr David Martin’s deposition (54)Dr David Martin’s deposition: https://odysee.com/@thecrowhouse:2/Brighteon:5
- Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China (55)Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7159299/
- Pollution comparisons (56)Pollution comparisons: https://www.numbeo.com/pollution/compare_cities.jsp?country1=Switzerland&country2=China&city1=Zurich&city2=Wuhan&tracking=getDispatchComparison
- Pneumonia Incidence and Mortality in Mainland China: Systematic Review of Chinese and English Literature, 1985–2008 (57)Pneumonia Incidence and Mortality in Mainland China: Systematic Review of Chinese and English Literature, 1985–2008: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0011721
- Notes from the Field: A Novel Coronavirus Genome Identified in a Cluster of Pneumonia Cases — Wuhan, China 2019−2020 (58)Notes from the Field: A Novel Coronavirus Genome Identified in a Cluster of Pneumonia Cases — Wuhan, China 2019−2020: http://weekly.chinacdc.cn/en/article/id/a3907201-f64f-4154-a19e-4253b453d10c
- Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR (59)Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR: https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.3.2000045
- Minimum Information for Publication of Quantitative Real-Time PCR Experiments (60)Minimum Information for Publication of Quantitative Real-Time PCR Experiments: https://www.gene-quantification.de/miqe-bustin-et-al-clin-chem-2009.pdf
- Dr Kelvin Watson’s PCR claim via OIA request (61)Dr Kelvin Watson’s PCR claim via OIA request: https://fyi.org.nz/request/14341/response/54651/attach/4/H202100581%20Virginia%20Crawford%20Response%20letter.pdf
- NZ Ministry of Health unable to provide evidence of their PCR claims (62)NZ Ministry of Health unable to provide evidence of their PCR claims: https://fyi.org.nz/request/15780-clinical-sensitivity-and-specificity-for-the-detection-of-sars-cov-2#comment-4053
- How much RNA does a typical mammalian cell contain? (63)How much RNA does a typical mammalian cell contain?: https://www.qiagen.com/us/resources/faq?id=06a192c2-e72d-42e8-9b40-3171e1eb4cb8&lang=en
- OffGuardian – PCR Inventor: “It doesn’t tell you that you are sick” (64)OffGuardian – PCR Inventor: “It doesn’t tell you that you are sick”: https://off-guardian.org/2020/10/05/pcr-inventor-it-doesnt-tell-you-that-you-are-sick/
- Identification of Coronavirus Isolated from a Patient in Korea with COVID-19 (65)Identification of Coronavirus Isolated from a Patient in Korea with COVID-19: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7045880/
Covid-19: Behind the PCR Curtain – Let’s dig deeper into PCR tests once again and have a look behind the curtain of this Covid-19 pandemic – Dr Sam Bailey (66)Covid-19: Behind the PCR Curtain – Dr Sam Bailey
- COVID-19 (Wikipedia) (67)COVID-19: https://en.wikipedia.org/wiki/COVID-19
- Claimed SARS-CoV-2 “Isolation”
Virus Isolation from the First Patient with SARS-CoV-2 in Korea (68)Park WB, Kwon NJ, Choi SJ, Kang CK, Choe PG, Kim JY, Yun J, Lee GW, Seong MW, Kim NJ, Seo JS, Oh MD. Virus Isolation from the First Patient with SARS-CoV-2 in Korea. J Korean Med Sci. 2020 Feb 24;35(7):e84. doi: 10.3346/jkms.2020.35.e84. PMID: … Click for full citation - Proof of SARS-CoV-2 225,000 EUR prize pool – “1 million € for a virologist who presents scientific proof of the existence of a corona virus, including documented control attempts of all steps taken in the proof.” (69)Proof of SARS-CoV-2 225,000 EUR prize pool Update: They have increased amount to: 1.5 million € for a virologist who provides scientific evidence of the existence of a corona virus. (70)Isolate Truth Fund – Updated
- Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR (71)Corman Victor M, Landt Olfert, Kaiser Marco, Molenkamp Richard, Meijer Adam, Chu Daniel KW, Bleicker Tobias, Brünink Sebastian, Schneider Julia, Schmidt Marie Luisa, Mulders Daphne GJC, Haagmans Bart L, van der Veer Bas, van den Brink Sharon, … Click for full citation
- Official recommendation of the Corman-Drosten protocol & manuscript by the WHO, published on January 13th 2020 as version 1.0 of the document: (72)Diagnostic detection of Wuhan coronavirus 2019 by real-time RTPCR – WHO – PDF (73)Diagnostic detection of Wuhan coronavirus 2019 by real-time RTPCR – WHO – PDF Archive.Org Backup (74)Diagnostic detection of Wuhan coronavirus 2019 by real-time RTPCR – WHO – PDF Archive.Org Backup – Shortlink/Bit.ly
- Corman-Drosten Review Report – Retraction request letter to Eurosurveillance editorial board (75)Corman-Drosten Review Report – Retraction request letter to Eurosurveillance editorial board
- COVID-19 test results and their accuracy – NZ Ministry of Health (76)COVID-19 test results and their accuracy – NZ Ministry of Health
- Analytical Specificity – NZ Ministry of Health (77)NZ Ministry of Health link to analytical specificity
- The MIQE Guidelines for PCR (Analytic specificity) (78)Bustin SA, Benes V, Garson JA, Hellemans J, Huggett J, Kubista M, Mueller R, Nolan T, Pfaffl MW, Shipley GL, Vandesompele J, Wittwer CT. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin Chem. … Click for full citation
- “A virus is just a piece of RNA molecule.” Prof Bill Rawlinson – Director of Virology NSW Health (ABC Broadcast 22 June 2020) (79)ABC Broadcast 22 June 2020, Prof Bill Rawlinson – Director of Virology NSW Health, “...a virus is just a piece of RNA molecule.”
- WHO COVID-19 Case definition update 16 December 2020 (80)WHO COVID-19 Case definition update 16 December 2020
- WHO SARS-CoV-2 PCR update 20 January 2021 (81)WHO SARS-CoV-2 PCR update 20 January 2021
- Landmark legal ruling finds that Covid tests are not fit for purpose. (82)Landmark legal ruling finds that Covid tests are not fit for purpose. So what do the MSM do? They ignore it
- Infectious Myth Podcast, David Crowe – Stephen Bustin on Challenges with RT-PCR 14 April 2020 (83)The Infectious Myth Podcast, David Crowe – Stephen Bustin on Challenges with RT-PCR 14 April 2020
- “It doesn’t tell you that you are sick” PCR Inventor (84)Off-Guardian 5 October 2020 – PCR Inventor: “It doesn’t tell you that you are sick”
Why Are Covid-19 Cases Soaring In NZ? PCR Test Update – Dr Sam Bailey talks about what is happening in NZ in regards to COVID-19 and important information you should know about the COVID-19 PCR Test.
- Professor Michael Baker on lockdown being an experiment. (85)Covid-19 coronavirus: NZ may have been spared worst-case disaster in ‘nick of time’ – expert: NZ Herald
- International Media Praising NZ 100 Days Covid Free (86)BBC – Coronavirus: New Zealand marks 100 days without community spread
- COVID pop up surveillance testing. (87) Hundreds of Cantabrians are tested for Covid-19 at pop-up facility – Stuff.NZ
- New Cases Unknown Source Ministry of Health: (88)Health.Gov.NZ – 4 cases of COVID-19 with unknown source
- Impact of Influenza Vaccination on Seasonal Mortality in the US Elderly Population. Arch Intern Med. 2005;165(3):265-272. (89)Impact of Influenza Vaccination on Seasonal Mortality in the US Elderly Population – 2005
- Vaccines for preventing influenza in the elderly. Cochrane Systematic Review 01 February 2018. (90)Vaccines for preventing influenza in the elderly – 2018
- 1918 Influenza: the Mother of All Pandemics. (91)Taubenberger JK, Morens DM. 1918 Influenza: the mother of all pandemics. Emerg Infect Dis. 2006;12(1):15-22. doi:10.3201/eid1201.050979
February 11 2021
Dr David Rasnick explains the PCR test on behalf of his friend, Kary Mullis (inventor of PCR)
Dr Dave Rasnick has a pHD in Chemistry and worked for nearly two decades in the pharmaceutical biotech industry, and was hired to set up the chemistry group in the diagnostics division of Abbott Laboratories where he learned learned a lot about clinical diagnostics, where a case used to be based on recognized and consistent clinical symptoms. He says technology is destroying disease diagnosis and is an advocate to revealing the truth to the public about what they don’t know about the pharmaceutical industry. (92) The Covid Vaccine On Trial: If You Only Knew… https://childrenshealthdefense.org/webinar/the-covid-vaccine-on-trial-if-you-only-knew-watch-now/ (93) David Rasnick PhD website https://www.davidrasnick.com/index.html (94) David Rasnick section / snippet on Rumble (mirror) https://rumble.com/v1o9gd7-dr-david-rasnick-calls-out-phony-pcr-testing-and-lies.html
In 1978, I was one of two PhDs hired to set up the chemistry group in the diagnostics division of Abbott Laboratories in north Chicago, Illinois. During my nearly two decades in the pharmaceutical biotech industry, I learned a lot about clinical diagnostics. Cases of cancer, flu, measles, alcoholism, etcetera, used to be based on clinical symptoms that are consistent and recognized for centuries. However, technology is in the process of destroying the very meaning of disease and how it’s diagnosed. Today, I want to talk about how the PCR test is being used to create cases of flu in people without symptoms of disease. As of January 3, 2020, the China office of the World Health Organization recorded 44 patients with pneumonia of unknown cause.
Just four days later, Fan Wu and colleagues in China claim they discovered a Coronavirus, a type of co-virus, in a 41-year-old man. It wasn’t long before that virus was officially declared the cause of those pneumonias. But here’s the question, what was so important about those 44 cases in a country that has over a million pneumonias every year? It is common knowledge that pneumonia can be caused by lots of things. Simply being older, medically compromised, or a patient in a hospital puts one at risk of developing pneumonia. Going from a handful of pneumonias to identifying a new virus from a single individual in a matter of days does not even come close to satisfying minimal scientific standards. It is very difficult and time-consuming to prove the existence of a new virus. It’s even more difficult to prove that it causes pneumonia or anything else, but it is impossible to do any of that if you don’t have authentic virus to begin with.
When virologist Charles Calisher at Colorado State University was asked last May if he knew of even one paper in which SARS-CoV-2 has been isolated and finding purified, his short email answer was, “I know of no such publication. I have kept an eye out for one.” Even the US Centers for Disease Control admitted in its December 1, 2020 update that, “No quantified virus isolates were available to validate the PCR test.” That’s right, the CDC does not have even a trace of virus to study and no one else does either. So what’s going on?
From the beginning, Wu and colleagues made the assumption that the man’s symptoms were caused by an infectious agent. When tests were negative for two viruses and a bacterium, they were committed to finding a virus causing his symptoms. They conducted a high-tech dragnet for all the RNA present in the man’s lung sample, but at no point did they work with actual infectious agents including viruses. Nowadays, it’s all technology and no biology. Wu and company used an extremely expensive and complicated new method called metatranscriptomics to pluck millions of RNA fragments from a sample taken from the lungs of that sick man. Then using a different array of very expensive high-tech machines, they determined the specific sequence of building blocks called nucleotides for each and every fragment of RNA in the sample. From the trillions of viruses that inhabit every one of us, including that sick man, a computer algorithm stitched together the nucleotide sequences into a string of RNA, characteristic of a family of cold viruses called Coronavirus.
Within days, China shared the computer-generated RNA sequence with other countries. Once the army of technologists around the world knew what to look for, almost overnight, the Wu sequence was merged with other constructed Coronavirus sequences to come up with what is called a consensus sequence, which was eventually christened SARS-CoV-2. Ultimately, this consensus sequence was used to develop PCR tests for a virus that the CDC doesn’t have. It is important to understand how the PCR test works because it is the only thing that keeps the phony Coronavirus pandemic going. Next slide, please.
In 1983, Kary Mullis invented PCR, which stands for polymerase chain reaction. In 1993, he got the Nobel Prize for PCR. PCR is like a photocopier that can make billions of copies of a single fragment of DNA. Kary and I first met through our mutual friend, Peter Duesberg, a professor at the University of California in Berkeley. In 1997, Peter, Kary, and I were invited to a meeting on AIDS in Colombia, South America. Kary explained why his truly amazing invention, PCR, cannot detect viruses in people or diagnose infections. Sadly, Kary Mullis died in August 2019, that’s why I’m here today instead of my friend. The genetic sequences of viruses, especially RNA viruses, are very unstable. So unstable, in fact, there is no such thing as an unmutated RNA virus. Viruses are like snowflakes, no two are identical.
An international database consortium based in Munich has already catalogued over 400,000 different sequences of SARS-CoV-2. Since SARS-CoV-2 exists only in computers, how does one go about making a PCR test to be used on human samples? It turns out that the most stable sequences of RNA viruses are approximately the same in all members of the viral family, including the family of coronaviruses. The 1% or less of the viral RNA that is amplified by the PCR test is chosen from these relatively stable samples. So at best, the PCR test is targeting a family of RNA viruses and not a specific virus. Before PCR can be done on the RNA of a coronavirus, a process that is error prone must first convert the RNA into DNA. By their very nature, the short synthetic sequences of DNA used to initiate each cycle of the PCR test cannot be guaranteed to distinguish between virus and non-virus. This alone makes PCR test highly suspect. However, these technical limitations were not the reason Kary opposed the PCR test. He simply could not accept equating a string of RNA or DNA with actual virus, Kary was not alone.
Charles Calisher, who works with real viruses has said, “Just studying genetic sequences is like trying to say whether somebody has bad breath by looking at his fingerprint. When asked, I tell people that using PCR to identify a virus is like conjuring up from a pile of bricks how a building looked before it was demolished.” Technologists have a bad habit of reading too much into genetic sequences. In the early days of genomics, researchers were shocked to discover that mice and humans both have virtually the same number of genes of which 99% are identical. Lisa Stubbs of the Lawrence Livermore National Laboratory said she knows of only a few cases in which no mouse counterpart can be found for a particular human gene and for the most part, we see essentially a one-to-one correspondence between the genes in the two species. Obviously, what makes a mouse a mouse and a human a human is not in the genes. The whole is not only more than, but decidedly different from the sum of its parts.
In spite of this obvious fact, many cell biologists and virtually all cancer researchers, diagnostics manufacturers, and drug developers believe they can understand, detect, and control living things one gene at a time. I and many other scientists are outraged by public officials using PCR testing to whip the public into a panic over COVID. With complete disregard for their oaths of office to uphold the Constitution and protect our liberties, politicians and public health authorities are using meaningless PCR testing results to justify lockdowns which are destroying lives, liberty, businesses, and society in general.
There are two things that keep the phony COVID pandemic going. The first is PCR testing. The second, you may have already guessed, is the endless flood of official propaganda and lies coming from government, departments of public health, and mainstream media. Public discussion, criticism, and debate are not permitted and in some places considered criminal. I want to stress that the PCR tests do not and cannot detect viruses, which means all PCR test results are meaningless. People should refuse PCR testing. If diagnostic PCR testing was stopped immediately, COVID would vanish into thin air and the highly dangerous vaccines can be incinerated. I would be honoured to strike the match.
Feb 28, 2021
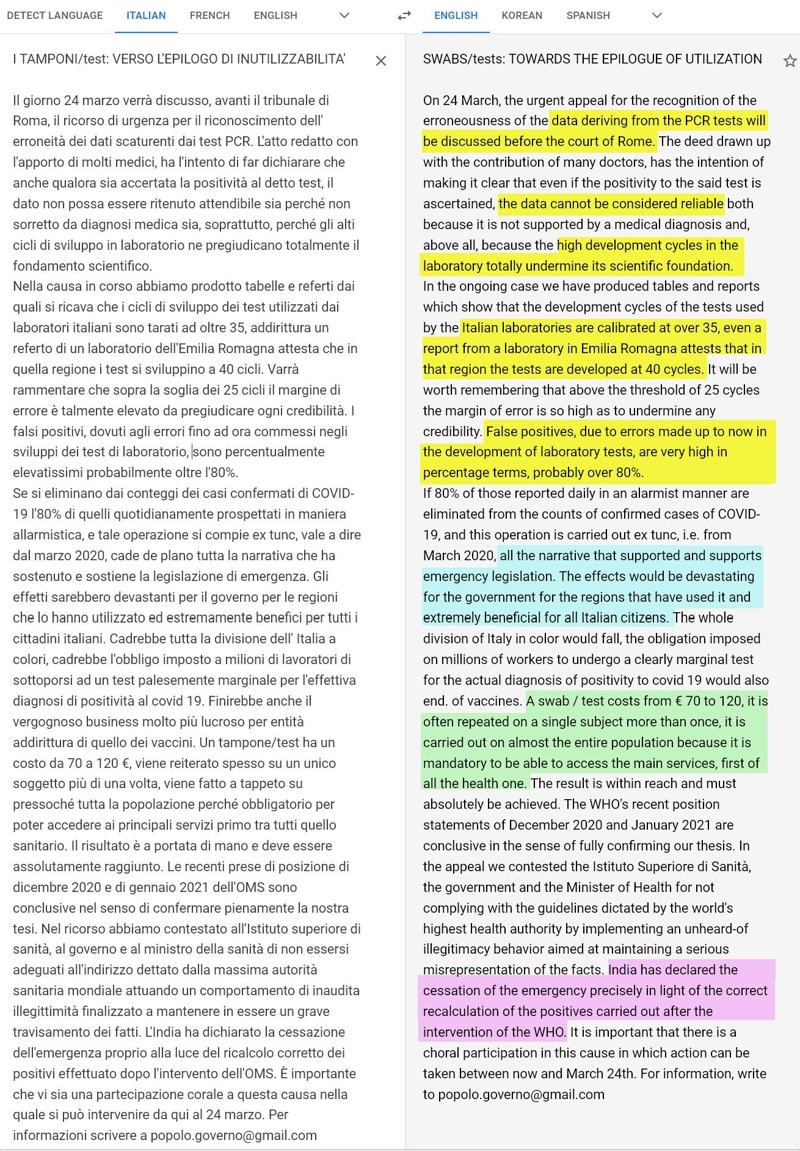
Italy appeal before the court of Rome to call out the government misusing PCR tests by having labs use cycles above 25 to give 80% false positives and keep the country under emergency powers to enforce vaccination and bring in the “Green Pass“. (95) Italy – Court Case about government misusing PCR tests. Follow Lawyer Mauro Sandri | See also YouTube video about case
SWABS/tests: TOWARDS THE EPILOGUE OF UTILIZATION
On 24 March, the urgent appeal for the recognition of the erroneousness of the data deriving from the PCR tests will be discussed before the court of Rome. The deed drawn up with the contribution of many doctors, has the intention of making it clear that even if the positivity to the said test is ascertained, the data cannot be considered reliable both because it is not supported by a medical diagnosis and, above all, because the high development cycles in the laboratory totally undermine its scientific foundation.
In the ongoing case we have produced tables and reports which show that the development cycles of the tests used by the Italian laboratories are calibrated at over 35, even a report from a laboratory in Emilia Romagna attests that in that region the tests are developed at 40 cycles. It will be worth remembering that above the threshold of 25 cycles the margin of error is so high as to undermine any credibility. False positives, due to errors made up to now in the development of laboratory tests, are very high in percentage terms, probably over 80%.
If 80% of those reported daily in an alarmist manner are eliminated from the counts of confirmed cases of COVID-19, and this operation is carried out ex tunc, i.e. from March 2020, all the narrative that supported and supports emergency legislation. The effects would be devastating for the government for the regions that have used it and extremely beneficial for all Italian citizens. The whole division of Italy in color would fall, the obligation imposed on millions of workers to undergo a clearly marginal test for the actual diagnosis of positivity to covid 19 would also end. of vaccines. A swab / test costs from € 70 to 120, it is often repeated on a single subject more than once, it is carried out on almost the entire population because it is mandatory to be able to access the main services, first of all the health one. The result is within reach and must absolutely be achieved. The WHO’s recent position statements of December 2020 and January 2021 are conclusive in the sense of fully confirming our thesis. In the appeal we contested the Istituto Superiore di Sanità, the government and the Minister of Health for not complying with the guidelines dictated by the world’s highest health authority by implementing an unheard-of illegitimacy behavior aimed at maintaining a serious misrepresentation of the facts. India has declared the cessation of the emergency precisely in light of the correct recalculation of the positives carried out after the intervention of the WHO. It is important that there is a choral participation in this cause in which action can be taken between now and March 24th. For information, write to popolo.governo@gmail.com
July 3 2021
Tonia Buxton – GBNews.uk – misspoke some numbers but shares the devastation the inaccurate PCR tests are causing which is unnecessarily creating a Two Tier Society (96)Vaccines will cause Two-Tier Society – Tonia Buxton – July 3 2021
- Claim:
“It’s a two-tier society – There’s lots of people that don’t want the jab, or can’t have the jab – and some people that don’t need the jab, there are some people brimming with antibodies and we’re not looking at that.” - Claim:
… “great concern about pushing vaccinations onto children that they don’t need..” - Claim:
… “Average Life-Expectancy in UK is 81.5 years
… “Average Age of those who “Died of COVID-19” is 82 years - Claim:
COVID-19 Blown way out of proportion: Scare-mongering. - Claim:
I’ll say a thousand times “These TESTS are NOT Correct” - Claim:
“Asymptomatic Tests done on 10 million people – Not just Rare – but “Impossible”
Locked away from our families on a ‘whim – on a guess’. - Claim:
“Suicides & Urgent Medical treatment delayed”
“More deaths caused by Lockdown than COVID-19”
Fact-Checked Claims to provide more accurate context (click title to expand)
- A majority of uninfected adults show pre-existing antibody reactivity against SARS-CoV-2 – Mar 15, 2021 (97)A majority of uninfected adults show preexisting antibody reactivity against SARS-CoV-2 | Abdelilah Majdoubi,Adrian B. McDermott, Pascal M. Lavoie, March 15, 2021 | JCI Insight. 2021;6(8):e146316.| https://doi.org/10.1172/jci.insight.146316
- A long-term perspective on immunity to COVID – Nature, 14 June 2021 (98)A long-term perspective on immunity to COVID – Nature, 14 June 2021
- SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study – Lancet (99)SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN) The Lancet – April 17, 2021
- Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection (100)Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection | Jennifer M. Dan, Jose Mateus, Yu Kato, Kathryn M. Hastie, Esther Dawen Yu, Caterina E. Faliti, Alba Grifoni, Sydney I. Ramirez, Sonya Haupt, April Frazier, Catherine … Click for full citation
- The durability of SARS-CoV-2 immunity after asymptomatic infection – May 3 2021 (101)Ross M. Kedl; Down but far from out: The durability of SARS-CoV-2 immunity after asymptomatic infection. J Exp Med 3 May 2021; 218 (5): e20210359. doi: https://doi.org/10.1084/jem.20210359
- Highly functional virus-specific cellular immune response in asymptomatic SARS-CoV-2 infection – May 3 2021 (102)Nina Le Bert, Hannah E. Clapham, Anthony T. Tan, Wan Ni Chia, Christine Y.L. Tham, Jane M. Lim, Kamini Kunasegaran, Linda Wei Lin Tan, Charles-Antoine Dutertre, Nivedita Shankar, Joey M.E. Lim, Louisa Jin Sun, Marina Zahari, Zaw Myo Tun, Vishakha … Click for full citation
- Mortality data & COVID-19 – March 28, 2021 – Joel Smalley (Quantitative Data Analyst) | PDF (103)Mortality data & COVID-19 – March 28, 2021 – Joel Smalley (Quantitative Data Analyst)
- The mortality profile of the covid-19 coronavirus is essentially zero for children and young adults
- near zero below 50
- begins to rise slowly and then very steeply above 70
- and especially above 80, reaching extreme levels in nursing homes. (104)Covid-19 Mortality: A Global Overview – Swiss Research
- Children’s immune responses seem to be able to eliminate the virus before it replicates in large numbers.” – How kids’ immune systems can evade COVID – Nature (105)Nogrady, Nature, December 2020
- Children are unlikely to cause household COVID-19 clusters or be major drivers of the pandemic even if attending school.
- Interventions aimed at children are expected to have a small impact on reducing SARS-CoV-2 transmission.” – Clinical Infectious Diseases, March 2021 (106)Antoni Soriano-Arandes, PhD, Anna Gatell, MD, Pepe Serrano, MD, Mireia Biosca, PhD, Ferran Campillo, MD, Ramon Capdevila, MD, Anna Fàbrega, MD, Zulema Lobato, MD, Núria López, MD/MSc, Ana Mª Moreno, MD, Miriam Poblet, MD, Maria Teresa … Click for full citation
- USA, UK, Italy, Germany, Spain, France, South Korea – deaths from COVID-19 in children remain rare up to February 2021, at 0.19 per 100 000 population, comprising 0.54% of the estimated total mortality from all causes in a normal year.” (107)Children and young people remain at low risk of COVID-19 mortality – Bhopal, The Lancet Child and Adolescent Health, March 2021
- Austria – Virus spreading from child-to-child in the same household seems to occur rarely.” (108)Austria – Lessons from low seroprevalence of SARS-CoV-2 antibodies in schoolchildren: A cross-sectional study” Szepfalusi, PAI, January 2021
- Germany – “Our investigation suggests that child-to-child transmission in schools and childcare facilities is uncommon and not the primary cause of SARS-CoV-2 infection in children.” (109)Germany -Citation style for this article: Ehrhardt J, Ekinci A, Krehl H, Meincke M, Finci I, Klein J, Geisel B, Wagner-Wiening C, Eichner M, Brockmann SO. Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools … Click for full citation
- Ireland: “No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020 (110)Ireland: “No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020 – Heavey, Eurosurveillance, May 2020
- Provisional COVID-19 Deaths: Focus on Ages 0-18 Years – CDC – July 1, 2021 (111)CDC – Provisional COVID-19 Deaths: Focus on Ages 0-18 Years – July 1, 2021
- Child mortality and COVID-19 – Unicef – Jan 2021 (112)Unicef – Child mortality and COVID-19 – Jan 2021
- COVID-19 Trends Among Persons Aged 0–24 Years — United States, March 1–December 12, 2020 – CDC -Jan 22, 2021 (113)CDC – COVID-19 Trends Among Persons Aged 0–24 Years — United States, March 1–December 12, 2020 – Jan 22, 2021
- Covid and Kids: The Evidence – Swiss Policy Research (114)Swiss Policy Research – Covid and Kids: The Evidence
- Comprehensive overview of paediatric COVID studies – DFTB portal (115)Boast A, Munro A, Goldstein H. An evidence summary of Paediatric COVID-19 literature, Don’t Forget the Bubbles, 2020. Available at: https://doi.org/10.31440/DFTB.24063
- COVID-19 vaccination in children – major ethical concerns | PDF (116)COVID-19 vaccination in children – major ethical concerns – March 17, 2021 – Dr Ros Jones – Retired Consultant Paediatrician
- Covid policies and harms to children | PDF (117)Covid policies and harms to children – March 17, 2021 – Dr Ros Jones (Retired Consultant Paediatrician) & Dr Zenobia Storah (Child and Adolescent Clinical Psychologist)
- UK – The average age of death for COVID-19 is 82.4, higher than the average age of death from other causes (81.5). (118)The average age of coronavirus fatalities is 82 – The Times – UK
- In most countries, the median age of covid deaths was close to the average life expectancy or even slightly above (e.g. 78 years in the USA and 80 to 86 years in western Europe).
- Therefore, despite high excess mortality in some countries, the temporary impact on life expectancy in 2020 was limited: it ranged from zero (in countries hardly affected by the coronavirus) to minus 2.1 years in US males: (119)Median age of Covid-19 deaths per country – Swiss Policy Research (120)Quantifying impacts of the COVID-19 pandemic through life expectancy losses José Manuel Aburto, Jonas Schöley, Luyin Zhang, Ilya Kashnitsky, Charles Rahal, Trifon I. Missov, Melinda … Click for full citation
- The covid-19 mortality profile is almost identical to natural mortality (121)Spiegelhalter D. Use of “normal” risk to improve understanding of dangers of covid-19 BMJ 2020; 370 :m3259 doi:10.1136/bmj.m3259
- Because of the covid-19 mortality profile, mass PCR testing and contact tracing in the general population make little sense and create an additional “casedemic” on top of the pandemic. (122)Because of the covid-19 mortality profile, mass PCR testing and contact tracing in the general population make little sense and create an additional “casedemic” on top of the pandemic.
Everything in this post backs up this claim. Here are some additional resources:
- A team of 22 international scientists published a review challenging the scientific paper on PCR testing for SARS-CoV-2 demanding it be retracted due to “fatal errors,”
- One of which is the fact that it was written, and the test itself developed, before any viral isolate was available.
- The test is simply based on a partial genetic sequence published online by Chinese scientists in January 2020. “China gave them a genetic sequence with no corresponding viral isolate to validate it”. (123)Review report Corman-Drosten et al. Eurosurveillance 2020
- This is the paper they are challenging – and is the very reason the entire globe is using PCR-Testing. (124)Corman Victor M, Landt Olfert, Kaiser Marco, Molenkamp Richard, Meijer Adam, Chu Daniel KW, Bleicker Tobias, Brünink Sebastian, Schneider Julia, Schmidt Marie Luisa, Mulders Daphne GJC, Haagmans Bart L, van der Veer Bas, van den Brink Sharon, … Click for full citation
- Test results are often misinterpreted, particularly if the prevalence of the condition being tested for is very low – British Medical Journal (125)Recchia G, Schneider CR, Freeman AL How do the UK public interpret COVID-19 test results? Comparing the impact of official information about results and reliability used in the UK, USA and New Zealand: a randomised … Click for full citation
- Fragments of inactive virus can be persistently detected by PCR in respiratory tract samples following infection – long after a person is no longer infectious. (126)COVID-19: management of staff and exposed patients or residents in health and social care settings – GOV.UK
- If you have no symptoms, your chances of being infectious and spreading the infection to others is basically nil. Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China – Nature.
- Of these, not a single person who had been in close contact with an asymptomatic individual ended up testing positive.
- This study even confirmed that even in cases where asymptomatic individuals had had an active infection, and had been carriers of live virus, the viral load had been too low for transmission. (127)Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China Cao, S., Gan, Y., Wang, C. et al. Nat Commun 11, 5917 (2020). https://doi.org/10.1038/s41467-020-19802-w
- No detectable live virus in patients after about seven days from onset of symptoms (at most 12 days).
- The PCR test, continued to register them as “positive” for SARS-CoV-2 for about 34 days.
- If you have no live virus in your body, you are not infectious and pose no risk to others.
- Viral culture was positive only in samples with a cycle-threshold value of 28.4 or less.
- The incidence of culture positivity decreased with an increasing time from symptom onset and with an increasing cycle-threshold value. – New England Journal of Medicine – Feb 18, 2021 (128)Duration of Culturable SARS-CoV-2 in Hospitalized Patients with Covid-19 – New England Journal of Medicine – Feb 18, 2021 | N Engl J Med 2021; 384:671-673 DOI: 10.1056/NEJMc2027040
- A study published back in April 2020 observed a significant relationship between Ct value and culture positivity rate.
- Samples with Ct values of 13–17 all led to positive culture.
- Culture positivity rate then decreased progressively according to Ct values to reach 12% at 33 Ct. (129)La Scola, B., Le Bideau, M., Andreani, J. et al. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur J Clin Microbiol Infect Dis 39, 1059–1061 (2020). … Click for full citation
- New report (Pre-Print) exposing the “1 in 3 people with Covid-19 have no symptoms” claim – What proportion of people with COVID-19 do not get symptoms? April 2021
- See also: YouTube summary (from the Author) of the Paper – Smashing the “1 in 3 people with Covid-19 have no symptoms” claim (130)Fenton, Norman & Neil, Martin & Mclachlan, Scott. (2021). What proportion of people with COVID-19 do not get symptoms?. 10.13140/RG.2.2.33939.60968. | Download PDF | YouTube Summary
- Only very weak studies show asymptomatic spread. Given that asymptomatic spread assumptions drive all of the other non-clinical interventions (mass-testing of healthy people, mandatory wearing of masks, social distancing and lockdowns), the evidence here must urgently be re-evaluated by policymakers. PDF (131)Asymptomatic spread: who can really spread COVID-19? Dr John Lee – Retired Professor of Pathology
- Lockdown makes a significant contribution to increases in death rates from non-Covid causes.
- Cancer, circulatory and heart disease, dementia were causes on death certificates and may have been prevented if patients had had normal access to doctors and hospitals. (132)Griffin S. Covid-19: “Staggering number” of extra deaths in community is not explained by covid-19 BMJ 2020; 369 :m1931 doi:10.1136/bmj.m1931
- Approximately one million excess deaths occurred in 2020 in 29 high income countries.
- Excess deaths substantially exceeded reported deaths from covid-19 in many countries, indicating that determining the full impact of the pandemic on mortality requires assessment of excess deaths. (133)Islam N, Shkolnikov V M, Acosta R J, Klimkin I, Kawachi I, Irizarry R A et al. Excess deaths associated with covid-19 pandemic in 2020: age and sex disaggregated time series analysis … Click for full citation
- A Peru study found a substantial drop in violent crime rates (close to 50% in some cities), and a reduction in traffic accidents, but an increase in domestic violence reports and suicides related to economic hardship as well as a result of the lockdown – Nov 2020 (134)Calderon-Anyosa RJC, Kaufman JS. Impact of COVID-19 lockdown policy on homicide, suicide, and motor vehicle deaths in Peru. Prev Med. 2021;143:106331. doi:10.1016/j.ypmed.2020.106331
- COVID-19-Related Suicides in Bangladesh Due to Lockdown and Economic Factors: Case Study Evidence from Media Reports (May, 2020): (135)Bhuiyan, A.K.M.I., Sakib, N., Pakpour, A.H. et al. COVID-19-Related Suicides in Bangladesh Due to Lockdown and Economic Factors: Case Study Evidence from Media Reports. Int J Ment Health Addiction (2020). … Click for full citation
- On 6 April, an adult man (aged 30 years) from Mohespur Upazila in Jhenaidah committed suicide (by hanging himself) due to the pressure of unpaid debts. In addition, his family was half-fed and had starved for a week after losing work after the lockdown and was denied any financial support from local government authorities (United News of Bangladesh 2020).
- On 10 April, a female adolescent (aged 10 years) from Belkuchi municipality of Sirajgonj committed suicide (by hanging herself) because she was rebuked by her father for asking for food. The lockdown meant that the girl’s father had to close his small loom factory and the family therefore had no money. The whole family had starved for a couple of days and they were also denied any financial relief from the local government authorities (Kaler Kantho 2020a).
- On 12 April, a woman and mother of five children (aged 35 years) from Cox’s Bazar attempted suicide by hanging, although one of her sons rescued her by getting help from her neighbors. Her husband lost his job because of the lockdown and they were also ineligible to receive relief goods from the local government authorities. The mother could not bear to see her starving children’s faces and thought that by killing herself she could provide more food for her starving children (Campus Today 2020).
- On 13 April, a young adult man (aged 27 years) from Noldangga village in Natore committed suicide (by hanging himself). He was a day laborer and he became unexpectedly unemployed as a result of the lockdown. He was struggling with starvation and to compound the situation, his wife also left him (prior to the pandemic) and the loneliness made his living situation worse (Kaler Kantho 2020b).
- On 14 April, a woman (whose age was not reported) from Dhamrai in Dhaka attempted suicide and kill her two children by setting themselves on fire with kerosene oil. Her husband became unemployed due to the shutdown of a garment factory where he worked and the mother was unable to work in a tea shop where she and her father-in-law worked. Consequently, the family experienced economic hardship. Additionally, she was asked by her father-in-law to leave the house with husband and children (RisingBD 2020a).
- On 16 April, an adult man (aged 30 years) from Bashkhali Upazila in Chattogram committed suicide (although no details of how were reported). The man was an auto-rickshaw driver and was unable to earn any money for his family because he was unable to use his vehicle to earn money during the lockdown. He approached the local government authorities for financial relief but was denied because they claimed there were other more deserving cases for financial help than his own (Daily Star 2020a).
- On 24 April, a poverty-stricken husband (aged 30 years) and wife (aged 24 years) from Keshapur committed suicide both hanging themselves from the roof of their house due to lockdown-related economic distress. The couple had a 3-year-old child and the family were very poor. The local government authority reported that the suicides were due to existing debts made worse by the national lockdown (Manab Zamin 2020).
- On 6 April, an adult man (aged 30 years) from Mohespur Upazila in Jhenaidah committed suicide (by hanging himself) due to the pressure of unpaid debts. In addition, his family was half-fed and had starved for a week after losing work after the lockdown and was denied any financial support from local government authorities (United News of Bangladesh 2020).
- Mother and Son Suicide Pact Due to COVID-19-Related Online Learning Issues in Bangladesh: An Unusual Case Report (136)Mamun, M.A., Chandrima, R.M. & Griffiths, M.D. Mother and Son Suicide Pact Due to COVID-19-Related Online Learning Issues in Bangladesh: An Unusual Case Report. Int J Ment Health Addiction (2020). … Click for full citation
- Alleged that a woman committed suicide at a hospital because she was not treated and because doctors and nurses suspected she was infected with COVID-19 and did not want to get infected themselves. Dec 2020 (137)Hospital suicide due to non-treatment by healthcare staff fearing COVID-19 infection in Bangladesh?
- Several Indian celebrities committed suicide during this COVID-19 pandemic: (138)Kar SK, Arafat SMY, Ransing R, et al. Repeated celebrity suicide in India during COVID-19 crisis: An urgent call for attention. Asian J Psychiatr. 2020;53:102382. doi:10.1016/j.ajp.2020.102382
- Ashutosh Bhakre on 30th July 2020.
- Actress Chandana, committed suicide on 28th May 2020 following relationship challenges
- Susheel Gowda, committed suicide in the first week of July 2020
- Sushant Singh Rajput (SSR), a popular mainstream Bollywood actor also committed suicide on June 14, 2020
- Two Tamil actors (Sreedhar & Jaya Kalyani) committed suicide in June 2020. These two actors were brother-sister were going through financial crisis due to lockdown related job loss
- A TV actor Manmeet Grewal also committed suicide by hanging due to stress of financial loss during this COVID-lockdown. It has been reported that people resisted themselves, to rescue the actor, when his wife shouted for help, due to the suspicion that the actor might have COVID-19 infection.
- 16 COVID-19 related suicide cases in one month in Pakistan.
- Most of the suicides occur due to lockdown-related economic recession.
- Fear of infection is the second suicide contributing factor.
- Lockdown-related unemployment aggravates the life-threatening situation. (139)Mamun MA, Ullah I. COVID-19 suicides in Pakistan, dying off not COVID-19 fear but poverty? – The forthcoming economic challenges for a developing country. Brain Behav Immun. 2020;87:163-166. doi:10.1016/j.bbi.2020.05.028
- 69 COVID-19 related suicide cases (aged 19 to 65 years; majority males) from Mar 27 2020 to May 18 2020. The suicide causalities are included as follows:
- fear of COVID-19 infection (n=21)
- followed by financial crisis (n=19)
- loneliness, social boycott and pressure to be quarantine
- COVID-19 positive
- COVID-19 work-related stress
- unable to come back home due to lockdown
- unavailability of alcohol etc. (140)Dsouza DD, Quadros S, Hyderabadwala ZJ, Mamun MA. Aggregated COVID-19 suicide incidences in India: Fear of COVID-19 infection is the prominent causative factor. Psychiatry Res. 2020;290:113145. doi:10.1016/j.psychres.2020.113145
- Couple-suicides and attempted suicides relating to COVID-19 from four countries (i.e., Bangladesh, India, Malaysia, and the US): (141)Griffiths MD, Mamun MA. COVID-19 suicidal behavior among couples and suicide pacts: Case study evidence from press reports. Psychiatry Res. 2020;289:113105. doi:10.1016/j.psychres.2020.113105
- (April 2, 2020; Source – BBC, 6 April 2020 ): An American couple from Lockport, Illinois – Patrick Jesernik (aged 54 years) and partner Cheryl Schriefer (aged 59) – were involved in a COVID-19-related murder-suicide by gunshot. Mr. Jesernik shot his partner (who had been suffering from severe breathing problems) before killing himself. He was scared that he had been infected with COVID-19 from his girlfriend. Both had been tested for COVID-19 but it appears neither had received their results before their deaths. The autopsies showed that neither was infected with COVID-19.
- (April 2, 2020: Source – Hindustan Times, 6 April 2020 ): An Indian elderly couple from Amritsar, India – Balwinder Singh (aged 65) and his wife Gurinder Kaur (age not reported) – committed suicide by consuming a poisonous substance together. Their suicide note said there was tension because of COVID-19. Their suicide note simply said: “We are finishing our lives. No one is responsible for this. There has been a tension due to coronavirus. We both were also ill”. The police reported they were not actually infected with COVID-19.
- (April 4, 2020: Source – New Indian Express, 5 April 2020 ): At Tiruchy International Airport, India, a Malaysian couple – Subramaniam (aged 65) and his wife Lalitha (aged 55) – both attempted suicide together by swallowing sleeping pills because they were not provided seats on a special COVID-19 rescue flight back to their home country of Malaysia. They were told by airport officials that their names were not listed on the flight and were dismayed by the responses from embassy officials and attempted to take their own lives. The suicide attempt was prevented by the police.
- (April 16, 2020: Source – Telegraph India, 17 April 2020 ): A young newlywed couple from Uttarakhand, India – Ashok Kumar (aged 24) and his wife Rajju Devi (age nor reported) – both committed suicide together by hanging themselves from a tree. Mr. Kumar was quarantined (after returning from Punjab) at a school that had been turned into an isolation center near his village. Although he had no COVID-19 symptoms, he was prevented from going home and his wife was being pressured and harassed by neighbors to leave the village because they all thought Mr. Kumar had COVID-19. The wife visited her husband at the quarantine center and both felt the situation was hopeless so committed suicide together in a forest nearby the center.
- (March 4, 2020: Source – Deccan Herald, 4 May 2020 ): A man from Bihar, India – Ramesh Shah (aged 35) – committed suicide by hanging himself after his wife (Suman, age not reported) committed suicide by setting herself on fire. The couple were unable to pay back a loan on a truck they had bought because they were unable to work during the COVID-19 lockdown. After an argument concerning their finances, Suman deliberately set herself on fire. The husband tried to save his wife but she died at hospital. The husband was so distraught that he then killed himself. The couple left behind two young children (aged 7 and 10)
- (April 2, 2020; Source – BBC, 6 April 2020 ): An American couple from Lockport, Illinois – Patrick Jesernik (aged 54 years) and partner Cheryl Schriefer (aged 59) – were involved in a COVID-19-related murder-suicide by gunshot. Mr. Jesernik shot his partner (who had been suffering from severe breathing problems) before killing himself. He was scared that he had been infected with COVID-19 from his girlfriend. Both had been tested for COVID-19 but it appears neither had received their results before their deaths. The autopsies showed that neither was infected with COVID-19.
- Lockdowns serve no useful purpose and cause catastrophic societal and economic harms. (Reviewing the data) Health Advisory & Recovery Team, UK (142)COVID-19: an overview of the evidence – HART – March 18, 2021
- Ethical considerations of the COVID-19 response – By Professor David Seedhouse (Professor of Deliberative Practice) | PDF – March 29, 2021 (143)Ethical considerations of the COVID-19 response – By Professor David Seedhouse (Professor of Deliberative Practice) – March 29, 2021
- Aged Care homes – we must do better for the most vulnerable in society – Dr Ali Haggett | PDF (144)Care homes – we must do better for the most vulnerable in society – Dr Ali Haggett – March 29, 2021 – Community mental health practitioner – older people
- Lockdowns have never previously been used in response to a pandemic.
- They have significant and serious consequences for health (including mental health), livelihoods and the economy.
- Around 21,000 excess deaths during the first UK lockdown alone were not COVID-19 deaths. These are people who would have lived had there not been a lockdown. (145)Williams, Sam and Crookes, Alasdair and Glass Kenjegalieva, Karligash and Glass, Anthony, An Improved Measure of Deaths Due to COVID-19 in England and Wales (June 25, 2020). Available at SSRN: https://ssrn.com/abstract=3635548 or … Click for full citation
- Millions impacted by reduced screening and assessment services across health conditions with many premature, avoidable deaths. (146)The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study – Camille Maringe, PhD, Prof James Spicer, PhD, Melanie Morris, PhD, Prof Arnie Purushotham, MD, Prof … Click for full citation (147)More than 24,000 cases of cancer have gone undiagnosed according to Cancer Research UK (148)Over 2 million people waiting for cancer screening, tests and treatments. Cancer Research UK, June 1, 2020
- Businesses have closed, never to reopen and livelihoods have been lost. (149)List of shops that have collapsed into administration in 2020 as UK lockdown hits high street
- Whilst the focus continues to stay primarily on COVID-19, the health of our nation is beleaguered by the collateral damage of this approach.
- In mental health, in elective surgeries cancelled and in the delicate structure of society. PDF (150)Lockdowns – do they work? March 28, 2021 – Professor Marilyn James (Professor of Health Economics) When an intervention has never been tried before, it is particularly important to carefully assess the potential harm it may inflict.
- Physical contact is essential for human beings. We are social animals. To deny people this for long and undefined periods causes enormous psychological and physical harm which we are clearly witnessing throughout the nation, in every corner of society. (151)Pagel JI, Choukèr A. Effects of isolation and confinement on humans-implications for manned space explorations. J Appl Physiol (1985). 2016 Jun 15;120(12):1449-57. doi: 10.1152/japplphysiol.00928.2015. Epub 2016 Feb 4. PMID: 26846554. (152)Cacioppo, J. T., & Cacioppo, S. (2014). Social Relationships and Health: The Toxic Effects of Perceived Social Isolation. Social and personality psychology compass, 8(2), 58–72. https://doi.org/10.1111/spc3.12087
- This is alongside the economic and societal implications, not to mention the long-term effects of lost educational years on our young people. (153)Davies, Neil M et al. “The Causal Effects of Education on Health Outcomes in the UK Biobank.” Nature human behaviour vol. 2,2 (2018): 117-125. doi:10.1038/s41562-017-0279-y
June 29 2021
PCR test cycles are different depending on vaccination status. Clip with Bret Weinstein and Heather Heying. June 29, 2021 (154)PCR test cycles are different depending on vaccination status. Clip with Bret Weinstein and Heather Heying.
- COVID-19 Vaccine Breakthrough Case Investigation and Reporting. Information for Health Departments. CDC: (Announcement) (155)CDC: COVID-19 Vaccine Breakthrough Case Investigation and Reporting. Information for Health Departments.
- Vaccine breakthrough (Information for state and local health departments) CDC: (PDF) (156)CDC: COVID-19 vaccine breakthrough case investigation. Information for state and local health departments (PDF)
- COVID-19 vaccine breakthrough case investigation CDC: (PDF) (157)CDC: COVID-19 vaccine breakthrough case investigation (PDF)
- Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. NY Times: (Article) (158)NY Times: Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.
- Q&A section between Bret Weinstein & Heather Heying Odysee: (Video) (159)Odysee: Q&A section between Bret Weinstein & Heather Heying
- PCR test cycles are different depending on vaccination status. Clip with Bret Weinstein and Heather Heying. YouTube: (Video)
- Bret’s website: (https://bretweinstein.net) (160)Bret Weinstein Website – https://bretweinstein.net
Dec 11 2021
This is a longer video (51 minutes) that has compiled a lot of what we know about PCR and COVID testing over the past couple of years, but also goes into things that no other video on this page goes through as it has added the more unverifiable conspiracy-like in nature – that people are concerned about like collecting everyone’s DNA, as well as raising questions about whether the tests & shots have the ability to biologically change, tag, or poison us. The technocrats and their robotics, digital ID, and genocide, as well as sterilization and wanting all humans of the future to be created in a lab. Bill Gates. Quantum dots, hydrogel, etc. It also shows a RAT test showing positive with tap water.
- DisclosureHub Videos: Rumble | Telegram
- VAULT (Vermonters Against Unconstitutional Lockdowns & Tyranna) VTValut.org
- Telegram Channels:
- In-Video Links (videos):
2020
September 9 2020
Positive PCR Test. Is It Really Positive? Drbeen Medical Lectures (161)Positive PCR Test. Is It Really Positive? Drbeen Medical Lectures
The screenshot DrBeen took in Sept 2020 of the CDC document, was updated Mar 16, 2021 (162)Interim Guidance on Ending Isolation and Precautions for Adults with COVID-19 – Mar 16, 2021 with the following:
Recommendations
- Duration of isolation and precautions
- For most adults with COVID-19 illness, isolation and precautions can be discontinued 10 days after symptom onset* and after resolution of fever for at least 24 hours, without the use of fever-reducing medications, and with improvement of other symptoms.
- Some adults with severe illness may produce replication-competent virus beyond 10 days that may warrant extending duration of isolation and precautions for up to 20 days after symptom onset; severely immunocompromised patients** may produce replication-competent virus beyond 20 days and require additional testing and consultation with infectious diseases specialists and infection control experts.
- For adults who never develop symptoms, isolation and other precautions can be discontinued 10 days after the date of their first positive RT-PCR test result for SARS-CoV-2 RNA.
- For most adults with COVID-19 illness, isolation and precautions can be discontinued 10 days after symptom onset* and after resolution of fever for at least 24 hours, without the use of fever-reducing medications, and with improvement of other symptoms.
- Role of viral diagnostic testing (RT-PCR or antigen)***to discontinue isolation or precautions
- For adults who are severely ill or severely immunocompromised, a test-based strategy could be considered in consultation with infectious diseases experts.
- For all others, who are not severely ill or severely immunocompromised, a test-based strategy is not recommended, and isolation and precautions should be maintained for at least 10 days as outlined in Part 1 above.
- Viral diagnostic testing (RT-PCR or antigen)***and quarantine after discontinuation of isolation or precautions
- For adults previously diagnosed with symptomatic laboratory-confirmed COVID-19 who remain asymptomatic after recovery, retesting or quarantine is not recommended if another exposure occurs or might have occurred within 90 days after the date of symptom onset from the initial SARS-CoV-2 infection.
- For adults who develop new symptoms consistent with COVID-19 during the 90 days after the date of initial symptom onset, if an alternative etiology cannot be readily identified by a healthcare provider, then the adult likely warrants retesting. Consultation with infectious disease or infection control experts is recommended, especially in the event that symptoms develop within 14 days after close contact with a person infected with SARS-CoV-2. Adults being evaluated for reinfection with SARS-CoV-2 or any potentially transmissible respiratory infection should be isolated under recommended precautions before and during evaluation. If reinfection is confirmed or remains suspected, they should remain under the recommended SARS-CoV-2 isolation period until they meet the criteria for discontinuation of precautions – for most adults, this would be 10 days after symptom onset and after resolution of fever for at least 24 hours, without the use of fever-reducing medications, and with improvement of other symptoms.
- For adults with past laboratory-confirmed SARS-CoV-2 who have never had symptoms and have had a subsequent exposure or possible exposure, the date of first positive viral diagnostic test result (RT-PCR or antigen) for SARS-CoV-2 should be used in place of the date of symptom onset to determine the interval between past infection and the recent exposure. This interval can then be used to inform decisions about testing for the recent exposure.
- Adults who have a past history of symptoms consistent with COVID-19 but who did not have laboratory confirmation of COVID-19 with a viral diagnostic test (RT-PCR or antigen) and who present with new symptoms consistent with COVID-19 should be tested and undergo quarantine.
- For children and infants, the data pertaining to the risk of reinfection within 90 days following laboratory-confirmed diagnosis are extremely limited. However, in the context of a pandemic, children and infants should be managed as recommended for adults above. CDC will continue to monitor closely the evolving science for information that would warrant reconsideration of these recommendations for this population.
- Role of serologic testing
- Although serologic testing indicating the presence of SARS-CoV-2 antibodies may signify resolving or previous infection, it should not generally be used to establish the presence or absence of acute SARS-CoV-2 infection. In addition, the date of a positive serologic test should not generally be used to determine the start of the 90-day period following SARS-CoV-2 infection for which retesting or quarantine is not recommended. However, if no positive viral diagnostic test (RT-PCR or antigen) indicating infection is available, a positive serologic test 7 days to 3 weeks following acute illness onset in an adult with a history of a previous negative serologic test can be used to establish the presence of absence of infection and the start date of the 90-day period.
- Interim Guidance on Ending Isolation and Precautions for Adults with COVID-19 CDC (163)Interim Guidance on Ending Isolation and Precautions for Adults with COVID-19 CDC
- US CDC Real-Time Reverse Transcription PCR Panel for Detection of Severe Acute Respiratory Syndrome Coronavirus 2 CDC: August 2020 (164)Lu X, Wang L, Sakthivel SK, Whitaker B, Murray J, Kamili S, et al. US CDC Real-Time Reverse Transcription PCR Panel for Detection of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg Infect Dis. 2020;26(8):1654-1665. … Click for full citation
- Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. NY Times: (Article) (165)NY Times: Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.
- Fast, Less-Accurate Coronavirus Tests May Be Good Enough. NY Times: (Article) (166)Fast, Less-Accurate Coronavirus Tests May Be Good Enough. NY Times
- C.D.C.’s ‘Clarification’ on Coronavirus Testing Offers More Confusion. NY Times: (Article) (167)C.D.C.’s ‘Clarification’ on Coronavirus Testing Offers More Confusion. NY Times
- Positive PCR Test. Is It Really Positive? Drbeen Medical Lectures (YouTube)
July 17 2020
The PCR-COVID test run at 36 cycles or higher is ‘dead nucleotides’. Interview with Dr Anthony Fauci – July 17, 2020 (168)Fauci PCR>36 Dead Nucleotides – Interview – 17 Jul 2020
So that if somebody – and you know what we do – we have patients, and it’s very frustrating for the patients – as well as for the physicians – somebody comes in, and they repeat their PCR, and it’s like 37 cycle-threshold, but you never – you can almost never can culture virus from a 37 threshold cycle.
So I think if somebody does come in with 37, 38, even 36. you gotta say y’know it’s just …it’s just dead nucleotides, period.”Anthony Fauci - 17 Jul 2020
- YouTube: Full Interview – July 17 2020 (03:54-5:45) (169)TWiV 641: COVID-19 with Dr. Anthony Fauci – 17 July 2020
- Rumble: Fauci PCR>36 Dead Nucleotides Quote (170)Fauci PCR>36 Dead Nucleotides – Interview – 17 Jul 2020
April 15 2020
Professor Stephen Bustin is an expert on quantitative PCR, and his research focuses on translating molecular techniques into practical, robust and reliable tools for clinical and diagnostic use. In this interview, he talks about the Challenges with RT-PCR (171) YouTube Version: The Infectious Myth Podcast, David Crowe – Stephen Bustin on Challenges with RT-PCR 14 April 2020
RT-PCR is the main method for declaring that someone is COVID-19 infected or not, as well as having numerous other uses in molecular biology research and biological testing.
Professor Stephen Bustin is a world expert on the technology, and the potential problems with using it to produce accurate and repeatable results.
Although the coronavirus test is presented as a binary test, it is actually based on whether the production of DNA is detectable prior to an arbitrary number of PCR cycles.
If there is variability in the quantification, then samples will be above or below the limit, when they should not be, resulting in false positives and negatives.
David and Stephen walk through the steps, from the extraction of RNA from the original sample, the conversion of the RNA to complementary DNA, and duplication of DNA using PCR, and the optional step of sequencing.
While this is dense technical information at times, it is presented logically, and the limitations of this method cannot be understood without taking the cover off the black box.
- Professor Stephen Bustin A.R.U. (172)Professor Stephen Bustin A.R.U.
- Stephen Bustin – Twitter (173)Stephen Bustin – Twitter
- Definitive qPCR – website (174)Definitive qPCR – website
- All Publications by Stephen Bustin on NCBI (175)All Publications by Stephen Bustin on NCBI
- COVID-19 and Diagnostic Testing for SARS-CoV-2 by RT-qPCR-Facts and Fallacies (176)Bustin S, Mueller R, Shipley G, Nolan T. COVID-19 and Diagnostic Testing for SARS-CoV-2 by RT-qPCR-Facts and Fallacies. Int J Mol Sci. 2021 Feb 28;22(5):2459. doi: 10.3390/ijms22052459. PMID: 33671091; PMCID: PMC7957603.
- RT-qPCR Testing of SARS-CoV-2: A Primer (177)Bustin SA, Nolan T. RT-qPCR Testing of SARS-CoV-2: A Primer. Int J Mol Sci. 2020 Apr 24;21(8):3004. doi: 10.3390/ijms21083004. PMID: 32344568; PMCID: PMC7215906.
Kary Mullis (Inventor of PCR)
Kary Mullis (1944 – 2019) PhD, Biochemist, invented & patented the PCR-test. He actually won a Nobel Prize because of the technology. (178)1993 Nobel Laureate in Chemistry, for the invention of the polymerase chain reaction (PCR) technique.
40 Second Video: The polymerase chain reaction (PCR) technique as explained in an older film on AIDS by Gary Null (2007) (179)Full Documentary “AIDS Inc. by Gary Null – 2007 – YouTube (180)Rumble Link – PCR Technique as explained in older AIDS film
This revolutionary technique allows scientists to take a sample containing a very minute amount of DNA and replicate that DNA sequence until there are many copies. One of the first applications of PCR was to analyze human tissue to detect the presence of HIV. PCR is commonly used in medical and biological research labs for the detection of virus culture in infectious persons.
Kary Mullis (inventor of PCR-Test) answers: “How do they misuse PCR to estimate all these supposed free viral RNA’s that may or may not be there?“ (181)Kary Mullis explains the PCR test (182)Kary Mullis Speaks To Misuse Of PCR (1993)
Dr Kary Mullis was not a fan of the CDC or Anthony Fauci who he says “does not mind going on television in front of the people, face out, and lie directly into the camera“. (183)Kary Mullis on Fauci
What is it about humanity that it wants to go to the all detail to stop and listen. Guys like Fauci get up there and start talking, and he doesn’t know anything really about anything, and I’d say that to his face. Nothing.
The man thinks you can take a blood sample and stick it in an electron microscope and if it’s got a virus in there, you will know it. He doesn’t understand electron microscopy and he doesn’t understand medicine. He should not be in a position like he’s in.
Most of those guys up there on the top are just total administrative people and they don’t know anything about what’s going on with the bottom. You know, those guys have got an agenda, which is not what we would like them to have, being that we pay for them to take care of our health in some way.
They’ve got a personal kind of agenda. They make up their own rules as they go. They change them when they want to and a smugly like Tony Fauci does not mind going on television in front of the people, face out, and lie directly into the camera.
You can’t expect the sheep to really respect the best and the brightest. They don’t know the difference, really. I mean, I like humans, don’t get me wrong. But basically, there is a vast, vast majority of them do not possess the ability to judge who is and who isn’t really a good scientist.
That’s a problem, that’s a main problem actually with science, I’d say, in this century. Because science is being judged by people. Funding is being done by people who don’t understand it. Who do we trust? Fauci? Fauci doesn’t know nothing, you know.
If Fauci wants to get on television with somebody who knows a little bit about this stuff and debate him, he could easily do it because he’s been asked. And I’ve had a lot of people… President of the University of South Carolina asked Fauci if he can come down there and debate me on the stage in front of the student body because I wanted somebody who was from the other side to come down and balance my point, because I felt like, “Well, these guys can listen to me but I need to have somebody else down here that’s going to tell me the other side.” But he didn’t want to do it. (184) Kary Mullis on Fauci
They’ve got a personal kind of agenda. They make up their own rules as they go. They change them when they want to and a smugly like Tony Fauci does not mind going on television in front of the people, face out, and lie directly into the camera.
PCR came about right about the same time as HIV: (185) Kary Mullis Interview – Clip 5 PCR came about right about the same time that HIV did
Kary Mullis: “the number of cases went up for HIV because the number of tests went up” (186)Kary Mullis Interview – Clip 6 Number of cases of HIV went up epidemically because the number of tests that was done went up exponentially
Kary Mullis compares the lab-coat-scientists on TV to something of a religion in its own right: (187)Fauci’s white robes
Watch the full interview: (188)Full Interview – Kary Mullis interviewed by Dr Gary Null – 1996 (189)Kary Mullis Interview – Transcripts & Backup Links
Videos I haven’t yet added references to:
- Jan 9 2021 – Dr.David Rasnick-PCR Test – David William Rasnick, PhD is an American biochemist with over 40 years experience, 20 years in the pharmaceutical/biotech industry.
- Feb 12 2021 – Dr David Rasnick – PCR Test Meaningless
- PCR Test Breakdown
In a ‘Pandemic of Lies‘ from ‘Official Sources’, you need to learn to do your own Research, stop getting your education from the corrupt media, stop trusting the corrupt health regulators, Question Everything. Wake up to the corruption.
PCR COVID-19 ( search results for site: pubmed.ncbi.nlm.nih.gov )
(yet to sort through and correctly interpret / date & cite – unknown if any of these are relevant)
- RT-PCR/MALDI-TOF mass spectrometry-based detection of SARS-CoV-2 in saliva specimens.
J Med Virol. 2021 May 8. doi: 10.1002/jmv.27069. - Stability issues of RT-PCR testing of SARS-CoV-2
In this study, we collected a total of 610 hospitalized patients from Wuhan between February 2, 2020, and February 17, 2020. We reported a potentially high false negative rate of real-time reverse-transcriptase polymerase chain reaction (RT-PCR) testing for SARS-CoV-2 in the 610 hospitalized patients clinically diagnosed with COVID-19 during the 2019 outbreak. - Dynamic profile of RT-PCR findings from 301 COVID-19 Patients
This large-scale investigation with 1113 RT-PCR test results from 301 COVID-19 patients showed that the average contagious period of SARS-CoV-2 infected patients was 20 days. Longer observation period and more than 2 series of negative viral test are necessary for patients ≥65 years. - Real-time RT-PCR in COVID-19 detection: issues affecting the results
In conclusion, according to the mentioned reasons, the results of real-time RT-PCR tests must be cautiously interpreted. In the case of real-time RT-PCR negative result with clinical features suspicion for COVID-19, especially when only upper respiratory tract samples were tested, multiple sample types in different time points, including from the lower respiratory tract if … - Diagnosing COVID-19: The Disease and Tools for Detection
Due to the shortage of kits and false negative rate of RT-PCR, the Hubei Province, China temporarily used CT scans as a clinical diagnosis for COVID-19. 47 Chest CT scans are non-invasive and involve taking many X-ray measurements at different angles across a patient’s chest to produce cross-sectional images. - The impact of false positive COVID-19
The UK’s COVID-19 testing programme uses real-time reverse transcription polymerase chain reaction (RT-PCR) tests to detect viral RNA. 1 Public Health England reports that RT-PCR assays show a specificity of over 95%, meaning that up to 5% of cases are false positives. 2 The impact of false positive results includes risk of overestimating the COVID-19 incidence, the demand on track … - SARS-CoV-2 Testing | COVID-19 Treatment Guidelines
(https://www.covid19treatmentguidelines.nih.gov/overview/sars-cov-2-testing/)
Testing for SARS-CoV-2 Infection. Summary Recommendations. To diagnose acute infection of SARS-CoV-2, the COVID-19 Treatment Guidelines Panel (the Panel) recommends using a nucleic acid amplification test (NAAT) with a sample collected from the upper respiratory tract (i.e., a nasopharyngeal, nasal, or oropharyngeal specimen) - NCBI Insights : Novel coronavirus complete genome from the …
Get rapid access to Wuhan coronavirus (2019-nCoV) sequence data from the current outbreak as it becomes available. We will continue to update the page with newly released data. The complete annotated genome sequence of the novel coronavirus associated with the outbreak of pneumonia in Wuhan, China is now available from GenBank for free and easy… - The Relationship Between Positivity for COVID-19 RT-PCR …
This study aimed to assess the correlation between nucleic acid amplification test (real-time reverse transcription-polymerase chain reaction, RT-PCR) positivity of patients presenting with suspected COVID-19 and pneumonic infiltration consistent with COVID-19-specific pneumonia diagnosis on thoracic computed tomography (CT), with symptoms, laboratory findings, and clinical … - Systematic screening for COVID-19 associated
From all adult COVID-19 patients admitted to the intensive care unit (ICU), TA samples were collected twice a week for Aspergillus screening by PCR and or culture. Bronchoalveolar lavage (BAL) sampling was performed in patients with a positive screening result if possible.
- PCR tests cannot determine an acute infection, ongoing infectiousness, and actual disease, especially if ct values are not taken into account. – The Trouble With PCR Tests – Swiss Policy Research (190)The Trouble With PCR Tests – Swiss Policy Research
- A French Study has shown that when the PCR test is run at 25 cycles, about 70% of samples were genuinely positive (infectious). However, when the test is run at a threshold of 30 cycles, only 20% of samples were infectious. At 35 cycles, only three percent of samples were infectious. And when run above 35 cycles – Zero samples were infectious.. (191)Rita Jaafar, Sarah Aherfi, Nathalie Wurtz, Clio Grimaldier, Thuan Van Hoang, Philippe Colson, Didier Raoult, Bernard La Scola, Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including … Click for full citation
- Several studies have since shown that national PCR testing rates have had no influence at all on covid mortality. (192)A Cross-Country Analysis of the Determinants of COVID-19 Fatalities – 23 Apr 21
- A study published in June, 2021 re-analyzed PCR tests of 160,000 people and concluded “In light of our findings that more than half of individuals with positive PCR test results are unlikely to have been infectious”. (193)Stang A, Robers J, Schonert B, Jöckel KH, Spelsberg A, Keil U, Cullen P. The performance of the SARS-CoV-2 RT-PCR test as a tool for detecting SARS-CoV-2 infection in the population. J Infect. 2021 Jun 1:S0163-4453(21)00265-6. doi: … Click for full citation
- Many US labs work with 35 to 45 cycles, (194)NY Times 35-45 Cycles while many European labs work with 30 to 40 cycles. (195)European Labs 30-40 Cycles
- Kevin McKernan – R&D lead Human Genome Project at MIT/WIBR – The Live-Dead qRT-PCR problem, the testing industrial complex and its impact on society. I never thought the work I did for the human genome project would be weaponized to lock down society. We are now ruled by qPCR right and the transparency on the process is shameful. (196)The Live-Dead qRT-PCR problem, the testing industrial complex and its impact on society. Kevin McKernan – R&D lead Human Genome Project at MIT/WIBR (197)Kevin on Twitter
- FDA document, May 19, 2021: FDA Advises Against Use of SARS-CoV-2 Antibody Test Results to Evaluate Immunity or Protection From COVID-19, Including After Vaccination – FDA Press Release (198)FDA document, May 19, 2021: FDA Advises Against Use of SARS-CoV-2 Antibody Test Results to Evaluate Immunity or Protection From COVID-19, Including After Vaccination – FDA Press Release
- From the New York Times Exposé: “I’m shocked that people would think that 40 could represent a positive,” she said. Julia Morrison, a virologist at the University of California. “A more reasonable cutoff would be 30 to 35“. Harvard epidemiologist, Dr. Michael Mina: “upwards of 90% of positive tests in Massachusetts with a 40 Ct threshold would have been negative at 30 Ct” (199)NY Times: Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.
- For those that don’t have access to the NY Times Exposé where they contacted various labs, interviewed virologists, and did an analysis on what is considered positive and informed the public to the fact that it could be 90% false-positive reporting: Response from Yale PDF Summary from Yale (200)Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. – NY Times Expose 29 Aug 2020 – PDF Summary
- The CDC was still recommending 40 cycles as recently as December 1, 2020. (201)PDF: CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel
- British Medical Journal – Dec 2020 found that 58% of positive tests at the University of Birmingham were false positives. (202)Armstrong S. Covid-19: Tests on students are highly inaccurate, early findings show BMJ 2020; 371 :m4941 doi:10.1136/bmj.m4941
- COVID-19 positive cases down 62% since World Health Organization updated PCR guidance – Feb 21, 2021
- A study published May 2020 reported no positive viral cultures with a Ct > 24. (203)Jared Bullard, Kerry Dust, Duane Funk, James E Strong, David Alexander, Lauren Garnett, Carl Boodman, Alexander Bello, Adam Hedley, Zachary Schiffman, Kaylie Doan, Nathalie Bastien, Yan Li, Paul G Van Caeseele, Guillaume Poliquin, Predicting … Click for full citation
- The Kansas Department of Health and Environment’s Health and Environmental Laboratories reduced (204)Screengrab of PCR recommendations changing from 42 to 35 – KDHE quietly reduced cycle threshold on COVID tests – Jan 21, 2021 the cycle threshold for its real-time COVID-19 test from 42 to 35 cycles. In October of 2020, KHEL said their most commonly-used test “has a Ct cutoff of 42 and is the most sensitive assay [test] currently available.” On January 7 2021, the Ct cutoff was changed to 35, and the last half of that sentence omitted.(205) SARS-CoV-2/COVID-19 virus PCR Ct Cutoff Values – Kansas Dept Health
- “Cycle thresholds between 12 and 36 are considered positive; results between 36 and 40 cycles are considered marginally positive, and anything over 40 cycles is considered negative.” – Bioningentech Manual (one of the manufacturers of the COVID PCR-Tests)
- Corman-Drosten Review Report – Curated By An International Consortium Of Scientists In Life Sciences (Icsls) [Nov 2020 – Jan 2021] – External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results. (206)Corman-Drosten Review Report
- The failure of PCR mass testing – Swiss Policy Research (207)The failure of PCR mass testing – Swiss Policy Research

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:


References[+]
| 01 | 2 Minute 101 on PCR-Tests |
|---|---|
| 02, 190 | The Trouble With PCR Tests – Swiss Policy Research |
| 03, 191 | Rita Jaafar, Sarah Aherfi, Nathalie Wurtz, Clio Grimaldier, Thuan Van Hoang, Philippe Colson, Didier Raoult, Bernard La Scola, Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates, Clinical Infectious Diseases, Volume 72, Issue 11, 1 June 2021, Page e921, https://doi.org/10.1093/cid/ciaa1491 |
| 04 | A Cross-Country Analysis of the Determinants of COVID-19 Fatalities – 23 Apr 21 |
| 05, 193 | Stang A, Robers J, Schonert B, Jöckel KH, Spelsberg A, Keil U, Cullen P. The performance of the SARS-CoV-2 RT-PCR test as a tool for detecting SARS-CoV-2 infection in the population. J Infect. 2021 Jun 1:S0163-4453(21)00265-6. doi: 10.1016/j.jinf.2021.05.022. Epub ahead of print. PMID: 34081958; PMCID: PMC8166461. |
| 06, 198 | FDA document, May 19, 2021: FDA Advises Against Use of SARS-CoV-2 Antibody Test Results to Evaluate Immunity or Protection From COVID-19, Including After Vaccination – FDA Press Release |
| 07 | Archive.org backup of Live-Dead qRT-PCR problem Thread by Kevin McKernan |
| 08 | The Live-Dead qRT-PCR problem |
| 09 | Threadreader: Kevin McKernan – R&D lead Human Genome Project at MIT/WIBR |
| 10 | Follow Kevin on Twitter |
| 11 | Threadreader: Kevin McKernan: But but… you ran it to 40-45 cycles? |
| 12 | Threadreader: Kevin McKernan: “Zero evidence of asymptomatic spread. |
| 13 | Threadreader: Kevin McKernan: Cliff Notes of 4 papers that Dissolve the Corman-Drosten RT-qPCR test. |
| 14 | Threadreader: Kevin McKernan: It’s frightening that no one seems to care about the Nuremberg code. Let’s walk through how many of these tenets are violated each day with qPCR testing of asymptomatic people and quarantining them on the results of such opaque tools. |
| 15 | Threadreader: Kevin McKernan: Now that we’ve gone over Nuremberg….Lets have a look at the published massive scale psychological experiment Facebook performed on its customers. |
| 16 | Threadreader: Kevin McKernan: This is the Final nail in the coffin of the current qPCR testing strategy. |
| 17 | Threadreader: Kevin McKernan: We have written another 60 page dissection of the Drosten PCR protocol. This should end all of the criticism of the initial retraction request not having enough “wet-lab” proof. 20 peer reviewed papers showing catastrophic problems |
| 18, 158, 165, 199 | NY Times: Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. |
| 19, 194 | NY Times 35-45 Cycles |
| 20, 195 | European Labs 30-40 Cycles |
| 21, 200 | Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. – NY Times Expose 29 Aug 2020 – PDF Summary |
| 22 | CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel – FDA/CDC PDF |
| 23, 202 | Armstrong S. Covid-19: Tests on students are highly inaccurate, early findings show BMJ 2020; 371 :m4941 doi:10.1136/bmj.m4941 |
| 24, 203 | Jared Bullard, Kerry Dust, Duane Funk, James E Strong, David Alexander, Lauren Garnett, Carl Boodman, Alexander Bello, Adam Hedley, Zachary Schiffman, Kaylie Doan, Nathalie Bastien, Yan Li, Paul G Van Caeseele, Guillaume Poliquin, Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples, Clinical Infectious Diseases, Volume 71, Issue 10, 15 November 2020, Pages 2663–2666, https://doi.org/10.1093/cid/ciaa638 |
| 25, 204 | Screengrab of PCR recommendations changing from 42 to 35 – KDHE quietly reduced cycle threshold on COVID tests – Jan 21, 2021 |
| 26, 205 | SARS-CoV-2/COVID-19 virus PCR Ct Cutoff Values – Kansas Dept Health |
| 27, 206 | Corman-Drosten Review Report |
| 28, 207 | The failure of PCR mass testing – Swiss Policy Research |
| 29 | PCR Testing | Planet Lockdown Film |
| 30, 45 | Kary Mullis on the PCR: https://www.youtube.com/watch?v=iWOJKuSKw5c |
| 31 | PCR: The Good, The Bad and The Bustin – OCT 2021 |
| 32 | Stephen Andrew Bustin: https://www.researchgate.net/profile/Stephen-Bustin |
| 33, 51 | The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments: https://www.gene-quantification.de/miqe-bustin-et-al-clin-chem-2009.pdf |
| 34 | RT-qPCR—Facts and Fallacies: An Interview With Professor Stephen Bustin: https://www.technologynetworks.com/diagnostics/articles/rt-qpcrfacts-and-fallacies-an-interview-with-professor-stephen-bustin-346520 |
| 35 | WHO Director-General’s opening remarks at the media briefing on COVID-19 – 16 March 2020: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—16-march-2020 |
| 36 | Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19: https://onlinelibrary.wiley.com/doi/10.1002/jmv.25786 |
| 37 | Planet Waves FM Interview with Dr. Stephen Bustin – February 10, 2021: https://planetwaves.net/planet-waves-fm-interview-with-dr-stephen-bustin/ |
| 38 | COVID-19 and Diagnostic Testing for SARS-CoV-2 by RT-qPCR—Facts and Fallacies: https://arro.anglia.ac.uk/id/eprint/706392/6/Bustin_et_al_2021.pdf |
| 39 | Portuguese Court Rules PCR Tests “Unreliable” & Quarantines “Unlawful”: https://off-guardian.org/2020/11/20/portuguese-court-rules-pcr-tests-unreliable-quarantines-unlawful/ |
| 40 | Austrian court overturns judgment: PCR test not suitable for diagnosis: https://mainland.press/2021/04/02/austrian-court-overturns-judgment-pcr-test-not-suitable-for-diagnosis/ |
| 41 | Austrian court ruling on the PCR (German): https://wp.tagesstimme.com/wp-content/uploads/2021/03/Verwaltungsgericht_FPOe-Versammlung.pdf |
| 42 | Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction–Based SARS-CoV-2 Tests by Time Since Exposure: https://www.acpjournals.org/doi/10.7326/M20-1495 |
| 43 | The PCR Hustle – SEPT 2021 |
| 44 | Counties Manukau- What happens to your Covid-19 Test? https://www.countiesmanukau.health.nz/news/curious-about-what-happens-to-your-covid-19-test/ |
| 46 | Celia Farber ft. David Crowe, 7 April, 2020 https://uncoverdc.com/2020/04/07/was-the-covid-19-test-meant-to-detect-a-virus/ |
| 47 | Australian Covid Medical Network: https://www.covidmedicalnetwork.com/open-letters/first-do-no-harm.aspx |
| 48 | NZ’s Covid Leaderboard: https://www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-19-data-and-statistics/covid-19-current-cases |
| 49 | University of Otago – Coronavirus testing – how does it work?: https://www.otago.ac.nz/biochemistry/research/otago736925.html |
| 50 | Otago Biochemistry -How does RT-PCR work?: https://www.youtube.com/watch?v=MU8-zIZagBc |
| 52 | Planet Waves FM Interview with Stephen Bustin, conducted by Eric F. Coppolino: http://chironreturn.org/audio/210201-steve-bustin.mp3 |
| 53 | Once Upon A Time in Wuhan…. – JUL 2021 |
| 54 | Dr David Martin’s deposition: https://odysee.com/@thecrowhouse:2/Brighteon:5 |
| 55 | Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7159299/ |
| 56 | Pollution comparisons: https://www.numbeo.com/pollution/compare_cities.jsp?country1=Switzerland&country2=China&city1=Zurich&city2=Wuhan&tracking=getDispatchComparison |
| 57 | Pneumonia Incidence and Mortality in Mainland China: Systematic Review of Chinese and English Literature, 1985–2008: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0011721 |
| 58 | Notes from the Field: A Novel Coronavirus Genome Identified in a Cluster of Pneumonia Cases — Wuhan, China 2019−2020: http://weekly.chinacdc.cn/en/article/id/a3907201-f64f-4154-a19e-4253b453d10c |
| 59 | Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR: https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.3.2000045 |
| 60 | Minimum Information for Publication of Quantitative Real-Time PCR Experiments: https://www.gene-quantification.de/miqe-bustin-et-al-clin-chem-2009.pdf |
| 61 | Dr Kelvin Watson’s PCR claim via OIA request: https://fyi.org.nz/request/14341/response/54651/attach/4/H202100581%20Virginia%20Crawford%20Response%20letter.pdf |
| 62 | NZ Ministry of Health unable to provide evidence of their PCR claims: https://fyi.org.nz/request/15780-clinical-sensitivity-and-specificity-for-the-detection-of-sars-cov-2#comment-4053 |
| 63 | How much RNA does a typical mammalian cell contain?: https://www.qiagen.com/us/resources/faq?id=06a192c2-e72d-42e8-9b40-3171e1eb4cb8&lang=en |
| 64 | OffGuardian – PCR Inventor: “It doesn’t tell you that you are sick”: https://off-guardian.org/2020/10/05/pcr-inventor-it-doesnt-tell-you-that-you-are-sick/ |
| 65 | Identification of Coronavirus Isolated from a Patient in Korea with COVID-19: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7045880/ |
| 66 | Covid-19: Behind the PCR Curtain – Dr Sam Bailey |
| 67 | COVID-19: https://en.wikipedia.org/wiki/COVID-19 |
| 68 | Park WB, Kwon NJ, Choi SJ, Kang CK, Choe PG, Kim JY, Yun J, Lee GW, Seong MW, Kim NJ, Seo JS, Oh MD. Virus Isolation from the First Patient with SARS-CoV-2 in Korea. J Korean Med Sci. 2020 Feb 24;35(7):e84. doi: 10.3346/jkms.2020.35.e84. PMID: 32080990; PMCID: PMC7036342. |
| 69 | Proof of SARS-CoV-2 225,000 EUR prize pool |
| 70 | Isolate Truth Fund – Updated |
| 71 | Corman Victor M, Landt Olfert, Kaiser Marco, Molenkamp Richard, Meijer Adam, Chu Daniel KW, Bleicker Tobias, Brünink Sebastian, Schneider Julia, Schmidt Marie Luisa, Mulders Daphne GJC, Haagmans Bart L, van der Veer Bas, van den Brink Sharon, Wijsman Lisa, Goderski Gabriel, Romette Jean-Louis, Ellis Joanna, Zambon Maria, Peiris Malik, Goossens Herman, Reusken Chantal, Koopmans Marion PG, Drosten Christian. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25(3):pii=2000045. https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000045 |
| 72 | Diagnostic detection of Wuhan coronavirus 2019 by real-time RTPCR – WHO – PDF |
| 73 | Diagnostic detection of Wuhan coronavirus 2019 by real-time RTPCR – WHO – PDF Archive.Org Backup |
| 74 | Diagnostic detection of Wuhan coronavirus 2019 by real-time RTPCR – WHO – PDF Archive.Org Backup – Shortlink/Bit.ly |
| 75 | Corman-Drosten Review Report – Retraction request letter to Eurosurveillance editorial board |
| 76 | COVID-19 test results and their accuracy – NZ Ministry of Health |
| 77 | NZ Ministry of Health link to analytical specificity |
| 78 | Bustin SA, Benes V, Garson JA, Hellemans J, Huggett J, Kubista M, Mueller R, Nolan T, Pfaffl MW, Shipley GL, Vandesompele J, Wittwer CT. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin Chem. 2009 Apr;55(4):611-22. doi: 10.1373/clinchem.2008.112797. Epub 2009 Feb 26. PMID: 19246619. |
| 79 | ABC Broadcast 22 June 2020, Prof Bill Rawlinson – Director of Virology NSW Health, “...a virus is just a piece of RNA molecule.” |
| 80 | WHO COVID-19 Case definition update 16 December 2020 |
| 81 | WHO SARS-CoV-2 PCR update 20 January 2021 |
| 82 | Landmark legal ruling finds that Covid tests are not fit for purpose. So what do the MSM do? They ignore it |
| 83 | The Infectious Myth Podcast, David Crowe – Stephen Bustin on Challenges with RT-PCR 14 April 2020 |
| 84 | Off-Guardian 5 October 2020 – PCR Inventor: “It doesn’t tell you that you are sick” |
| 85 | Covid-19 coronavirus: NZ may have been spared worst-case disaster in ‘nick of time’ – expert: NZ Herald |
| 86 | BBC – Coronavirus: New Zealand marks 100 days without community spread |
| 87 | Hundreds of Cantabrians are tested for Covid-19 at pop-up facility – Stuff.NZ |
| 88 | Health.Gov.NZ – 4 cases of COVID-19 with unknown source |
| 89 | Impact of Influenza Vaccination on Seasonal Mortality in the US Elderly Population – 2005 |
| 90 | Vaccines for preventing influenza in the elderly – 2018 |
| 91 | Taubenberger JK, Morens DM. 1918 Influenza: the mother of all pandemics. Emerg Infect Dis. 2006;12(1):15-22. doi:10.3201/eid1201.050979 |
| 92 | The Covid Vaccine On Trial: If You Only Knew… https://childrenshealthdefense.org/webinar/the-covid-vaccine-on-trial-if-you-only-knew-watch-now/ |
| 93 | David Rasnick PhD website https://www.davidrasnick.com/index.html |
| 94 | David Rasnick section / snippet on Rumble (mirror) https://rumble.com/v1o9gd7-dr-david-rasnick-calls-out-phony-pcr-testing-and-lies.html |
| 95 | Italy – Court Case about government misusing PCR tests. Follow Lawyer Mauro Sandri | See also YouTube video about case |
| 96 | Vaccines will cause Two-Tier Society – Tonia Buxton – July 3 2021 |
| 97 | A majority of uninfected adults show preexisting antibody reactivity against SARS-CoV-2 | Abdelilah Majdoubi,Adrian B. McDermott, Pascal M. Lavoie, March 15, 2021 | JCI Insight. 2021;6(8):e146316.| https://doi.org/10.1172/jci.insight.146316 |
| 98 | A long-term perspective on immunity to COVID – Nature, 14 June 2021 |
| 99 | SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN) The Lancet – April 17, 2021 |
| 100 | Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection | Jennifer M. Dan, Jose Mateus, Yu Kato, Kathryn M. Hastie, Esther Dawen Yu, Caterina E. Faliti, Alba Grifoni, Sydney I. Ramirez, Sonya Haupt, April Frazier, Catherine Nakao, Vamseedhar Rayaprolu, Stephen A. Rawlings, Bjoern Peters, Florian Krammer, Viviana Simon, Erica Ollmann Saphire, Davey M. Smith, Daniela Weiskopf, Alessandro Sette, Shane Crotty | Science 05 Feb 2021 | Immune memory to SARS-CoV-2 is highly variable, but protection against reinfection and subsequent disease seems possible in most cases. |
| 101 | Ross M. Kedl; Down but far from out: The durability of SARS-CoV-2 immunity after asymptomatic infection. J Exp Med 3 May 2021; 218 (5): e20210359. doi: https://doi.org/10.1084/jem.20210359 |
| 102 | Nina Le Bert, Hannah E. Clapham, Anthony T. Tan, Wan Ni Chia, Christine Y.L. Tham, Jane M. Lim, Kamini Kunasegaran, Linda Wei Lin Tan, Charles-Antoine Dutertre, Nivedita Shankar, Joey M.E. Lim, Louisa Jin Sun, Marina Zahari, Zaw Myo Tun, Vishakha Kumar, Beng Lee Lim, Siew Hoon Lim, Adeline Chia, Yee-Joo Tan, Paul Anantharajah Tambyah, Shirin Kalimuddin, David Lye, Jenny G.H. Low, Lin-Fa Wang, Wei Yee Wan, Li Yang Hsu, Antonio Bertoletti, Clarence C. Tam; Highly functional virus-specific cellular immune response in asymptomatic SARS-CoV-2 infection. J Exp Med 3 May 2021; 218 (5): e20202617. doi: https://doi.org/10.1084/jem.20202617 |
| 103 | Mortality data & COVID-19 – March 28, 2021 – Joel Smalley (Quantitative Data Analyst) |
| 104 | Covid-19 Mortality: A Global Overview – Swiss Research |
| 105 | Nogrady, Nature, December 2020 |
| 106 | Antoni Soriano-Arandes, PhD, Anna Gatell, MD, Pepe Serrano, MD, Mireia Biosca, PhD, Ferran Campillo, MD, Ramon Capdevila, MD, Anna Fàbrega, MD, Zulema Lobato, MD, Núria López, MD/MSc, Ana Mª Moreno, MD, Miriam Poblet, MD, Maria Teresa Riera-Bosch, PhD, Neus Rius, MD/MSc, Montserrat Ruiz, MD, Almudena Sánchez, MD, Cinta Valldepérez, MD, Mònica Vilà, PhD, Valentí Pineda, PhD, Uxue Lazcano, MSc, Yesika Díaz, MSc, Juliana Reyes-Urueña, PhD, Pere Soler-Palacín, PhD, COPEDI-CAT research group, Household SARS-CoV-2 transmission and children: a network prospective study, Clinical Infectious Diseases, 2021;, ciab228, https://doi.org/10.1093/cid/ciab228 |
| 107 | Children and young people remain at low risk of COVID-19 mortality – Bhopal, The Lancet Child and Adolescent Health, March 2021 |
| 108 | Austria – Lessons from low seroprevalence of SARS-CoV-2 antibodies in schoolchildren: A cross-sectional study” Szepfalusi, PAI, January 2021 |
| 109 | Germany -Citation style for this article: Ehrhardt J, Ekinci A, Krehl H, Meincke M, Finci I, Klein J, Geisel B, Wagner-Wiening C, Eichner M, Brockmann SO. Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools after their reopening in May 2020, Baden-Württemberg, Germany. Euro Surveill. 2020;25(36):pii=2001587. https://doi.org/10.2807/1560-7917.ES.2020.25.36.2001587 |
| 110 | Ireland: “No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020 – Heavey, Eurosurveillance, May 2020 |
| 111 | CDC – Provisional COVID-19 Deaths: Focus on Ages 0-18 Years – July 1, 2021 |
| 112 | Unicef – Child mortality and COVID-19 – Jan 2021 |
| 113 | CDC – COVID-19 Trends Among Persons Aged 0–24 Years — United States, March 1–December 12, 2020 – Jan 22, 2021 |
| 114 | Swiss Policy Research – Covid and Kids: The Evidence |
| 115 | Boast A, Munro A, Goldstein H. An evidence summary of Paediatric COVID-19 literature, Don’t Forget the Bubbles, 2020. Available at: https://doi.org/10.31440/DFTB.24063 |
| 116 | COVID-19 vaccination in children – major ethical concerns – March 17, 2021 – Dr Ros Jones – Retired Consultant Paediatrician |
| 117 | Covid policies and harms to children – March 17, 2021 – Dr Ros Jones (Retired Consultant Paediatrician) & Dr Zenobia Storah (Child and Adolescent Clinical Psychologist) |
| 118 | The average age of coronavirus fatalities is 82 – The Times – UK |
| 119 | Median age of Covid-19 deaths per country – Swiss Policy Research |
| 120 | Quantifying impacts of the COVID-19 pandemic through life expectancy losses José Manuel Aburto, Jonas Schöley, Luyin Zhang, Ilya Kashnitsky, Charles Rahal, Trifon I. Missov, Melinda C. Mills, Jennifer B. Dowd, Ridhi KashyapmedRxiv 2021.03.02.21252772; doi: https://doi.org/10.1101/2021.03.02.21252772 |
| 121 | Spiegelhalter D. Use of “normal” risk to improve understanding of dangers of covid-19 BMJ 2020; 370 :m3259 doi:10.1136/bmj.m3259 |
| 122 | Because of the covid-19 mortality profile, mass PCR testing and contact tracing in the general population make little sense and create an additional “casedemic” on top of the pandemic. |
| 123 | Review report Corman-Drosten et al. Eurosurveillance 2020 |
| 124 | Corman Victor M, Landt Olfert, Kaiser Marco, Molenkamp Richard, Meijer Adam, Chu Daniel KW, Bleicker Tobias, Brünink Sebastian, Schneider Julia, Schmidt Marie Luisa, Mulders Daphne GJC, Haagmans Bart L, van der Veer Bas, van den Brink Sharon, Wijsman Lisa, Goderski Gabriel, Romette Jean-Louis, Ellis Joanna, Zambon Maria, Peiris Malik, Goossens Herman, Reusken Chantal, Koopmans Marion PG, Drosten Christian. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25(3):pii=2000045. https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000045 Received: 21 Jan 2020; Accepted: 22 Jan 2020 |
| 125 | Recchia G, Schneider CR, Freeman AL How do the UK public interpret COVID-19 test results? Comparing the impact of official information about results and reliability used in the UK, USA and New Zealand: a randomised controlled trialBMJ Open 2021;11:e047731. doi: 10.1136/bmjopen-2020-047731 |
| 126 | COVID-19: management of staff and exposed patients or residents in health and social care settings – GOV.UK |
| 127 | Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China Cao, S., Gan, Y., Wang, C. et al. Nat Commun 11, 5917 (2020). https://doi.org/10.1038/s41467-020-19802-w |
| 128 | Duration of Culturable SARS-CoV-2 in Hospitalized Patients with Covid-19 – New England Journal of Medicine – Feb 18, 2021 | N Engl J Med 2021; 384:671-673 DOI: 10.1056/NEJMc2027040 |
| 129 | La Scola, B., Le Bideau, M., Andreani, J. et al. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur J Clin Microbiol Infect Dis 39, 1059–1061 (2020). https://doi.org/10.1007/s10096-020-03913-9 |
| 130 | Fenton, Norman & Neil, Martin & Mclachlan, Scott. (2021). What proportion of people with COVID-19 do not get symptoms?. 10.13140/RG.2.2.33939.60968. | Download PDF | YouTube Summary |
| 131 | Asymptomatic spread: who can really spread COVID-19? Dr John Lee – Retired Professor of Pathology |
| 132 | Griffin S. Covid-19: “Staggering number” of extra deaths in community is not explained by covid-19 BMJ 2020; 369 :m1931 doi:10.1136/bmj.m1931 |
| 133 | Islam N, Shkolnikov V M, Acosta R J, Klimkin I, Kawachi I, Irizarry R A et al. Excess deaths associated with covid-19 pandemic in 2020: age and sex disaggregated time series analysis in 29 high income countries BMJ 2021; 373 :n1137 doi:10.1136/bmj.n1137 |
| 134 | Calderon-Anyosa RJC, Kaufman JS. Impact of COVID-19 lockdown policy on homicide, suicide, and motor vehicle deaths in Peru. Prev Med. 2021;143:106331. doi:10.1016/j.ypmed.2020.106331 |
| 135 | Bhuiyan, A.K.M.I., Sakib, N., Pakpour, A.H. et al. COVID-19-Related Suicides in Bangladesh Due to Lockdown and Economic Factors: Case Study Evidence from Media Reports. Int J Ment Health Addiction (2020). https://doi.org/10.1007/s11469-020-00307-y |
| 136 | Mamun, M.A., Chandrima, R.M. & Griffiths, M.D. Mother and Son Suicide Pact Due to COVID-19-Related Online Learning Issues in Bangladesh: An Unusual Case Report. Int J Ment Health Addiction (2020). https://doi.org/10.1007/s11469-020-00362-5 |
| 137 | Hospital suicide due to non-treatment by healthcare staff fearing COVID-19 infection in Bangladesh? |
| 138 | Kar SK, Arafat SMY, Ransing R, et al. Repeated celebrity suicide in India during COVID-19 crisis: An urgent call for attention. Asian J Psychiatr. 2020;53:102382. doi:10.1016/j.ajp.2020.102382 |
| 139 | Mamun MA, Ullah I. COVID-19 suicides in Pakistan, dying off not COVID-19 fear but poverty? – The forthcoming economic challenges for a developing country. Brain Behav Immun. 2020;87:163-166. doi:10.1016/j.bbi.2020.05.028 |
| 140 | Dsouza DD, Quadros S, Hyderabadwala ZJ, Mamun MA. Aggregated COVID-19 suicide incidences in India: Fear of COVID-19 infection is the prominent causative factor. Psychiatry Res. 2020;290:113145. doi:10.1016/j.psychres.2020.113145 |
| 141 | Griffiths MD, Mamun MA. COVID-19 suicidal behavior among couples and suicide pacts: Case study evidence from press reports. Psychiatry Res. 2020;289:113105. doi:10.1016/j.psychres.2020.113105 |
| 142 | COVID-19: an overview of the evidence – HART – March 18, 2021 |
| 143 | Ethical considerations of the COVID-19 response – By Professor David Seedhouse (Professor of Deliberative Practice) – March 29, 2021 |
| 144 | Care homes – we must do better for the most vulnerable in society – Dr Ali Haggett – March 29, 2021 – Community mental health practitioner – older people |
| 145 | Williams, Sam and Crookes, Alasdair and Glass Kenjegalieva, Karligash and Glass, Anthony, An Improved Measure of Deaths Due to COVID-19 in England and Wales (June 25, 2020). Available at SSRN: https://ssrn.com/abstract=3635548 or http://dx.doi.org/10.2139/ssrn.3635548 |
| 146 | The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study – Camille Maringe, PhD, Prof James Spicer, PhD, Melanie Morris, PhD, Prof Arnie Purushotham, MD, Prof Ellen Nolte, PhD, Prof Richard Sullivan, PhD, et al. July 20, 2020 DOI:https://doi.org/10.1016/S1470-2045(20)30388-0 |
| 147 | More than 24,000 cases of cancer have gone undiagnosed according to Cancer Research UK |
| 148 | Over 2 million people waiting for cancer screening, tests and treatments. Cancer Research UK, June 1, 2020 |
| 149 | List of shops that have collapsed into administration in 2020 as UK lockdown hits high street |
| 150 | Lockdowns – do they work? March 28, 2021 – Professor Marilyn James (Professor of Health Economics) When an intervention has never been tried before, it is particularly important to carefully assess the potential harm it may inflict. |
| 151 | Pagel JI, Choukèr A. Effects of isolation and confinement on humans-implications for manned space explorations. J Appl Physiol (1985). 2016 Jun 15;120(12):1449-57. doi: 10.1152/japplphysiol.00928.2015. Epub 2016 Feb 4. PMID: 26846554. |
| 152 | Cacioppo, J. T., & Cacioppo, S. (2014). Social Relationships and Health: The Toxic Effects of Perceived Social Isolation. Social and personality psychology compass, 8(2), 58–72. https://doi.org/10.1111/spc3.12087 |
| 153 | Davies, Neil M et al. “The Causal Effects of Education on Health Outcomes in the UK Biobank.” Nature human behaviour vol. 2,2 (2018): 117-125. doi:10.1038/s41562-017-0279-y |
| 154 | PCR test cycles are different depending on vaccination status. Clip with Bret Weinstein and Heather Heying. |
| 155 | CDC: COVID-19 Vaccine Breakthrough Case Investigation and Reporting. Information for Health Departments. |
| 156 | CDC: COVID-19 vaccine breakthrough case investigation. Information for state and local health departments (PDF) |
| 157 | CDC: COVID-19 vaccine breakthrough case investigation (PDF) |
| 159 | Odysee: Q&A section between Bret Weinstein & Heather Heying |
| 160 | Bret Weinstein Website – https://bretweinstein.net |
| 161 | Positive PCR Test. Is It Really Positive? Drbeen Medical Lectures |
| 162 | Interim Guidance on Ending Isolation and Precautions for Adults with COVID-19 – Mar 16, 2021 |
| 163 | Interim Guidance on Ending Isolation and Precautions for Adults with COVID-19 CDC |
| 164 | Lu X, Wang L, Sakthivel SK, Whitaker B, Murray J, Kamili S, et al. US CDC Real-Time Reverse Transcription PCR Panel for Detection of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg Infect Dis. 2020;26(8):1654-1665. https://doi.org/10.3201/eid2608.201246 |
| 166 | Fast, Less-Accurate Coronavirus Tests May Be Good Enough. NY Times |
| 167 | C.D.C.’s ‘Clarification’ on Coronavirus Testing Offers More Confusion. NY Times |
| 168, 170 | Fauci PCR>36 Dead Nucleotides – Interview – 17 Jul 2020 |
| 169 | TWiV 641: COVID-19 with Dr. Anthony Fauci – 17 July 2020 |
| 171 | YouTube Version: The Infectious Myth Podcast, David Crowe – Stephen Bustin on Challenges with RT-PCR 14 April 2020 |
| 172 | Professor Stephen Bustin A.R.U. |
| 173 | Stephen Bustin – Twitter |
| 174 | Definitive qPCR – website |
| 175 | All Publications by Stephen Bustin on NCBI |
| 176 | Bustin S, Mueller R, Shipley G, Nolan T. COVID-19 and Diagnostic Testing for SARS-CoV-2 by RT-qPCR-Facts and Fallacies. Int J Mol Sci. 2021 Feb 28;22(5):2459. doi: 10.3390/ijms22052459. PMID: 33671091; PMCID: PMC7957603. |
| 177 | Bustin SA, Nolan T. RT-qPCR Testing of SARS-CoV-2: A Primer. Int J Mol Sci. 2020 Apr 24;21(8):3004. doi: 10.3390/ijms21083004. PMID: 32344568; PMCID: PMC7215906. |
| 178 | 1993 Nobel Laureate in Chemistry, for the invention of the polymerase chain reaction (PCR) technique. |
| 179 | Full Documentary “AIDS Inc. by Gary Null – 2007 – YouTube |
| 180 | Rumble Link – PCR Technique as explained in older AIDS film |
| 181 | Kary Mullis explains the PCR test |
| 182 | Kary Mullis Speaks To Misuse Of PCR (1993) |
| 183 | Kary Mullis on Fauci |
| 184 | Kary Mullis on Fauci |
| 185 | Kary Mullis Interview – Clip 5 PCR came about right about the same time that HIV did |
| 186 | Kary Mullis Interview – Clip 6 Number of cases of HIV went up epidemically because the number of tests that was done went up exponentially |
| 187 | Fauci’s white robes |
| 188 | Full Interview – Kary Mullis interviewed by Dr Gary Null – 1996 |
| 189 | Kary Mullis Interview – Transcripts & Backup Links |
| 192 | A Cross-Country Analysis of the Determinants of COVID-19 Fatalities – 23 Apr 21 |
| 196 | The Live-Dead qRT-PCR problem, the testing industrial complex and its impact on society. Kevin McKernan – R&D lead Human Genome Project at MIT/WIBR |
| 197 | Kevin on Twitter |
| 201 | PDF: CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel |
Truth-seeker, ever-questioning, ever-learning, ever-researching, ever delving further and deeper, ever trying to 'figure it out'. This site is a legacy of sorts, a place to collect thoughts, notes, book summaries, & random points of interests.
DISCLAIMER: The information on this website is not medical science or medical advice. I do not have any medical training aside from my own research and interest in this area. The information I publish is not intended to diagnose, treat, cure or prevent any disease, disorder, pain, injury, deformity, or physical or mental condition. I just report my own results, understanding & research.
![“C-19 Jabs are bioweapons” [Karen Kingston] Florida County Commissioners Presentation](https://pennybutler.com/wp-content/uploads/2023/03/KarenKingston-FL-County-Presentation-777x400.jpg)
![Archbishop Viganò Addresses Australia [27 Feb 2022]](https://pennybutler.com/wp-content/uploads/2022/11/archbishop-australia.jpg)
![[RANT] People are still dying & hospitalized even after being ‘fully vaccinated’ (UK, Israel)](https://pennybutler.com/wp-content/uploads/2021/10/cognitivedissonance-777x437.jpg)