AHPRA
- Updated:1 year ago
- Reading Time:55Minutes
- Post Words:14677Words

Collating all the AHPRA resources.
Who, or what, is AHPRA?
A “monstrous bureaucracy” in Canberra that rules over all Australian health professionals including doctors, dentists, nurses, physiotherapists, paramedics, osteopaths, and pharmacists.
Living Document. First published May 13, 2022. Last updated March 24, 2023
2023
AHPRA forces Doctors to break informed consent
7 Mar 2023 YouTube “Doctors across Australia have told us that they’re being intimidated into complying with the so-called government health advice – even against their own judgement.” Senator Malcolm Roberts
AHPRA during Pandemic

We’ve all heard about it. The Australian Health Practitioner Regulation Agency (AHPRA) is engaged in an aggressive witch hunt against any Australian Health professional who deviates even slightly from the State-imposed Covid narrative.
- The AHPRA Inquisition Against Australian Health Professionals (external link)
Scott Morrison’s older brother, Alan, serves as Chair of AHPRA (Australian Health Practitioner Regulation Agency) Committee on Paramedicine and Chair of the government’s Health Services Working Group.
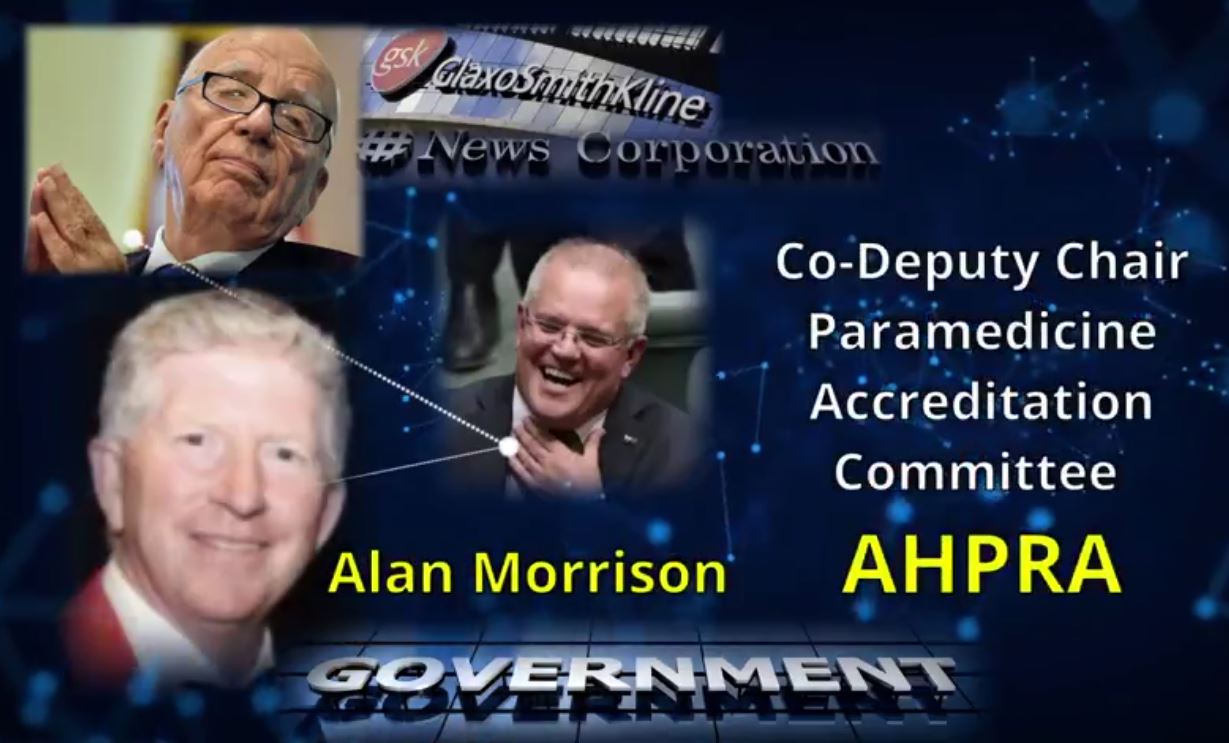
- Scott Morrison’s brother, Alan Morrison is Co-Deputy Chair at AHPRA
- AHPRA is the governing regulator that is directing health practitioners in Australia to promote the mRNA inoculations and reject Ivermectin and other COVID treatments.
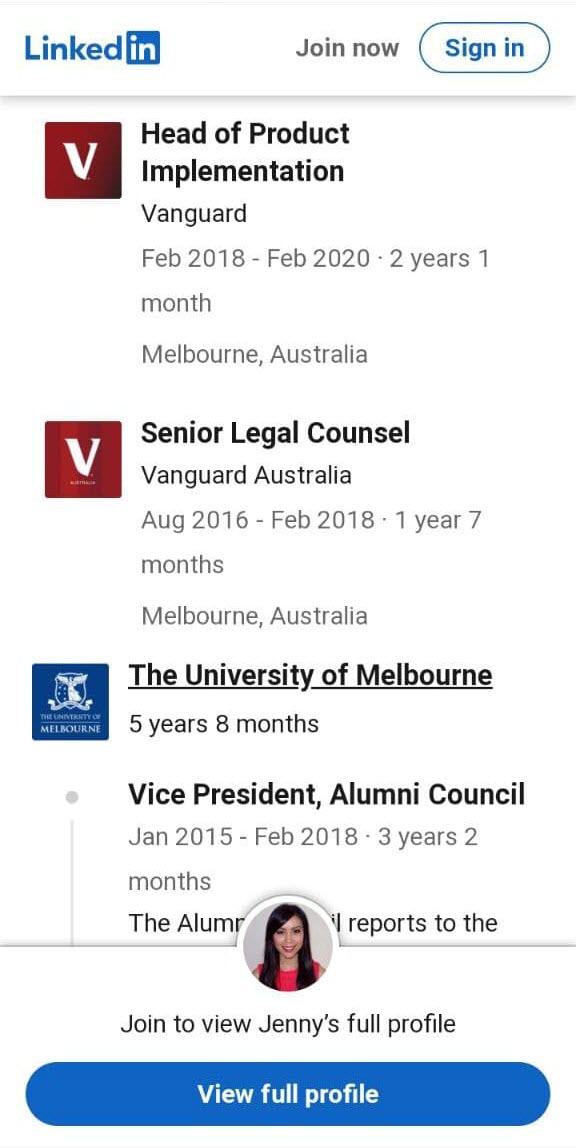
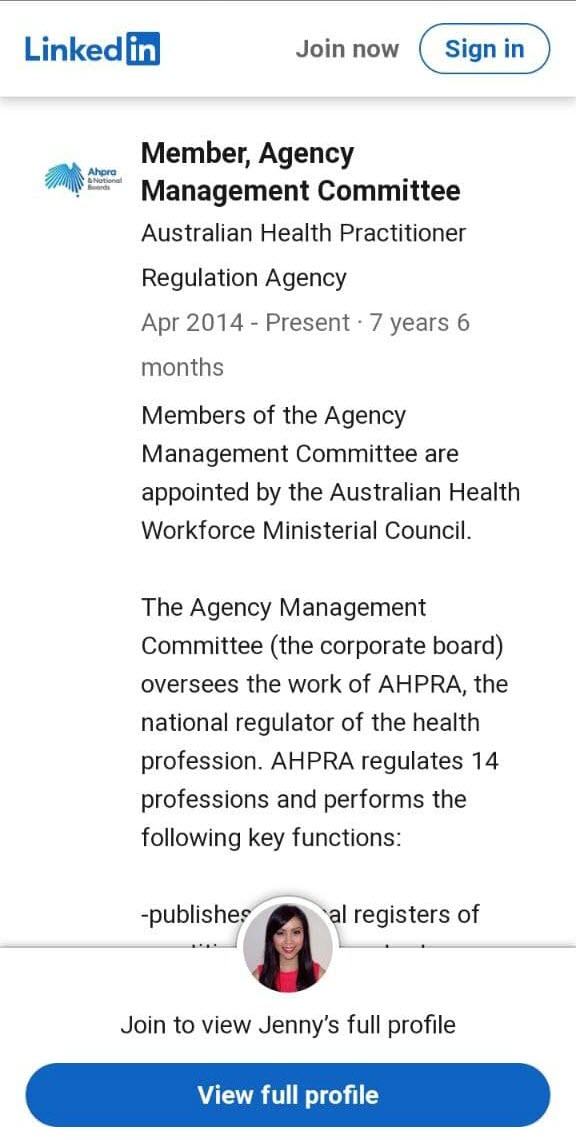
Jenny Taing
- Board Director of the Australian Health Practitioner Regulation Agency (AHPRA)
- Deputy Chair of the Western Bulldogs Football Club Community Foundation & member of the Western Bulldogs Football Club Ethics and Integrity Committee.
- ETHICS? INTEGRITY? (Bulldogs held Webinars to convince Parents to get their kids injected ignoring all known issues from official sources (health.gov.au, WHO, CDC, FDA) and only took questions from people that promoted the vaccine as safe & effective! They even made sure the webinar questions could only be seen by hosts!)
- Former Head of Product Implementation at Vanguard! !! !! *!!! @*($^!@ !!! WTF.
- Vanguard owns $16 Billion in Pfizer shares
- (Blackrock is Pfizer 2nd largest investor)
- (Vanguard & Blackrock Own the World)
- Former Lawyer at Australian Securities & Investments Commission !(!@!$@*() WTF.
Scroll images in lightbox:



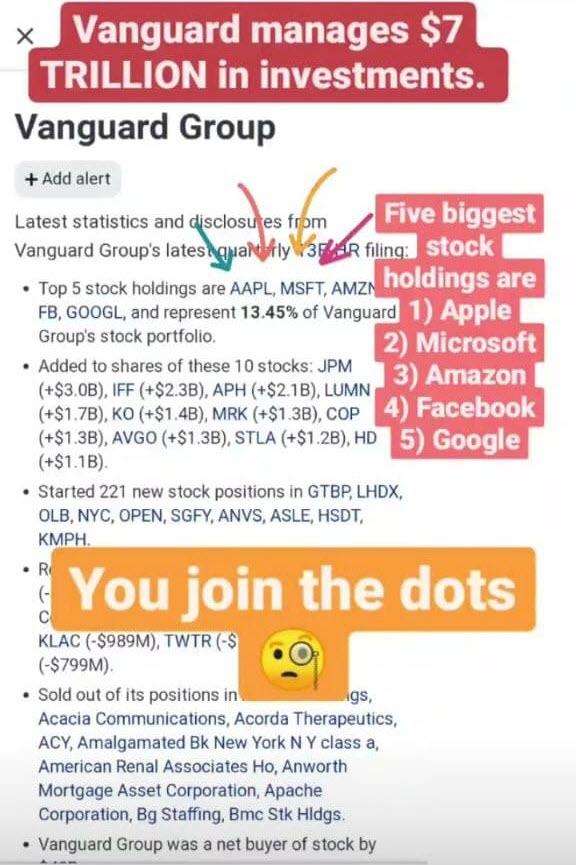
- Who Owns the World?
- Heart Damage: mRNA Vaccines (Pfizer/Moderna) (Watch the Western Bulldogs Webinar to try and get parents to get their kids jabbed … if you want to be disgusted with their ignorance!)
- AHPRA Member Profiles (external link)
- AHPRA Management Committee “Ms Jenny Taing… “senior lawyer with Vanguard Investments Australia and is a specialist in financial services, managed funds and superannuation law.” (external link)
- Transparency.gov.au Jenny Taing… “board director of the Australian Health Practitioner Regulation Agency (AHPRA)” (external link)
- Jenny Taing LinkedIn (external link)
- Jenny Taing Hive Legal (external link)
Unbelievable.
Can’t promote eating healthy without being deregistered (see 2016, 2017 sections below), but you can create promotions for experimental new injections?
Even offers of gifts, discounts or other inducements are permitted!
- AHPRA “Promotion of COVID-19 vaccinations: further information for healthcare practitioners and other advertisers” | (83.3 KB,PDF), (103 KB,DOCX) (external links)
Dr Mark Hobart raided & deregistered by AHPRA
Doctor Mark Hobart was raided by authorities without a warrant in November. They seized his patient files without his permission.
He has now been told by AHPRA he is not allowed to refer to himself as a doctor, as he will be facing 3 years in prison, or $60,000 per offence. The people have chosen to still refer to him as a doctor.
- Dr Mark Hobart raided & deregistered by AHPRA (Rumble) (external link)
- Dr Mark Hobart raided by Victorian Government 10-11-21 (YouTube) (external link)
- Support Dr Hobart (GiveSendGo) (external link)
- Posts tagged Dr Mark Hobart
Dr Judy Wilyman – AHPRA ‘Doctors Gagged from Speaking Up’
Covid Truth with Dr Judy Wilyman
- 4:45 For a decade I’ve watched as the government took control of the doctors, and silenced them through APRHA.
- 5:00 Doctors are required now to promote government-vaccination policies. They can no longer put the patients best interest first.
- 6:00 Doctor-Patient relationship has been hijacked by government policy. They are no longer abiding by their medical ethics and no longer giving fully-informed consent, without coercion, manipulation, or pressure. Which is the actual wording in the Australian Immunisation Handbook; which is the directives for doctors to give vaccines.
- 6:30 Violated medical ethics and principles of medicine. Every doctor is educated to know that you must give a drug to a person with advice regarding their own specific circumstances and genetics. There is no drug that you can give blanket to an entire genetically-diverse population.
- 8:45 The problem here is APRHA is actually a government board, and an incorporated business. Being a government board, it’s controlled by Ministers, who are actually designing vaccination policy.
- The Australian Government Regulates Medical Knowledge on Vaccines The corruption in the promotion of vaccines to the public was cemented in 2009 when a government board was set up in Australia to regulate doctors on the “accepted” science for vaccine promotion. This Federal government agency is called the Australian Health Practitioners Regulatory Authority (AHPRA) and it is both a government agency AND an Australian incorporated business (ABN 78 685 433 429). In other words, this board controls the knowledge doctors can promote on vaccines AND it influences the design and promotion of government vaccination policies. This board has the power to de-register doctors and health professionals who make a different risk assessment of vaccines to that provided by this government regulatory board.
- 9:00 So they have gagged doctors on the risks of vaccines, the chronic illnesses that can come out immediately or it could be months or years later. There is no scientific debate. You’re all getting ridiculed if you talk about risks of vaccines “that’s just an ‘anti-vaxxer'”, and doctors can be de-registered / removed from their practice if they present the risks of vaccines that I’ve discovered in the medical literature in my research.
- 10:00 The knowledge that doctors are given in medical school now. That education is funded by the pharmaceutical companies. So they’ve used selective-studies, and they use recent studies that have been designed – see an Epidemiology study – you can ‘choose the parameters of that study’ – so you can pretty well design any study to prove the outcome you want. When you see a study with a conclusion on it – unless you go back and look at the design of that study – you don’t know if that was an accurate conclusion or not.
- 11:00 This is the tragedy: Money is Power. Money is now controlling “education” and the school curriculums – the indoctrination in the education system teaching “vaccines controlled these diseases” – and they didn’t.
- 11:30 It’s the “Regulatory Board” that is preventing them from speaking about the true risk of vaccines, and even the benefits are exaggerated.
- 12:15 And with the Covid Injection Rollout- they didn’t even trial it for 1 year before they had it on the market. The trial IS the human population. Greg Hunt has told you that. The TGA has told you that. The Lawyers are telling you that.
- 12:30 Because this drug has been called a ‘vaccine’ – everybody is ‘conditioned’ by the word ‘vaccine’, and the public are not even investigating – they’re just walking in to get this drug that is actually new, untested genetic technology.
- 14:25 It’s not in their interest to find out because ethically – you can’t do your job comfortably once you are aware of the full knowledge of the risks and benefits of these vaccines. There’s also a lot of bonuses you get for giving injections – and they even get a lump sum for raising the vaccination rates of children. The money is controlling people’s behaviour.
- Against Our Will [Australia & New Zealand]
- Covid Truth with Dr Judy Wilyman (post with references)
- C-19 Vaccines [Videos] Doctors & Nurses
- Covid Truth with Dr Judy Wilyman (Rumble) (external link)
- Book based on her PhD research “Australia’s Loss of Health Freedom”
Nurse – Melbourne – Truth About COVID Vaccines & AHPRA
We have a bunch of unelected bureaucrats at AHPRA, none of whom have any experience in frontline medicine, gagging doctors, nurses and other allied health professionals to keep them from doing their job—from writing the very diagnosis that our injured need feedback on and that our community need feedback on so they know just how dangerous these vaccines are.
By gagging our medical professionals, AHPRA are stopping vaccine victims from getting the treatment and support they need, and they are stopping the rest of society from understanding just how dangerous these vaccines can be. It is completely unacceptable that AHPRA have bullied our medical professionals into silence. I should however acknowledge the many medical professionals who had the courage to speak out at great cost to themselves and to their families. Your efforts will not be forgotten.
We have people injured from the first vaccine or the second vaccine who can’t get an exemption from their next shot because doctors are afraid to write anything down. How cruel is that—to force someone to get a second vaccine after they’ve been injured from the first? What’s even worse is that many people who’ve been injured actually can’t get an exemption. Some get a medical exemption, but then they get the sack anyway. What is going on here? This is just unbridled abuse. I’ve heard these stories every day for the last five months. It has got to stop.
AHPRA’s bullying doesn’t just lead to poor treatment. It leads to further cover-ups, the worst being the underreporting of vaccine injuries. I know a cardiologist in Brisbane who lodged three reports of myocarditis from the vaccine with Queensland Health. They knocked the reports back, saying that the cardiologist wasn’t qualified to give an assessment on the condition of someone’s heart and that these vaccine victims had to go back to their GPs. Just how many adverse events are being underreported because of this systemic cover-up of vaccine-injuries, not just by Ahpra but also by our good friends at the TGA?
The Australian Health Practitioner Regulatory Agency (AHPRA), has been bullying medical practitioners into not reporting or even for talking about the harm they’re seeing. The TGA erased 98 per cent of the 800 vaccine deaths—98% erased!—that physicians reported. The TGA did so without autopsy or suitable consideration of all the patient medical data. TGA, ATAGI and AHPRA are the three monkeys of the pharmaceutical industry: hear no evil, see no evil, speak no evil.
- Mar 29, 2022: Mirror | Transcript | Hansard (external links)
- QLD Senator Malcolm Roberts: Website | COVID Under Question: A Cross-Party Inquiry (external links)
- QLD Senator: Truth Bombs “We won’t let you get away with it”
Senator Rennick calls for Australian health professionals to be able to openly speak about COVID policies without repercussions since they were gagged by “policy”. May 15, 2022

Medical Cover Up in Australia – Albany Doctor Speaks Out.
June 7, 2022 | Rumble
Interview: Dr. Mitch S. speaks out about how AHPRA (Australian Health Practitioners Regulation Agency) violated medical ethics in a cover up to hide increasing Jab injuries and deaths. All across Australia injuries and deaths have increased as result of unscientific medical (Jab) mandates. These deaths and injuries includes Pericarditis and Myopericarditis.
Senator Roberts expresses his disgust in the gagging of doctors by AHPRA, the forced coercion for Australians to receive injections that were not found to be either safe or effective / questioning why they haven’t been halted, and calls them out for being converted to a private corporation.
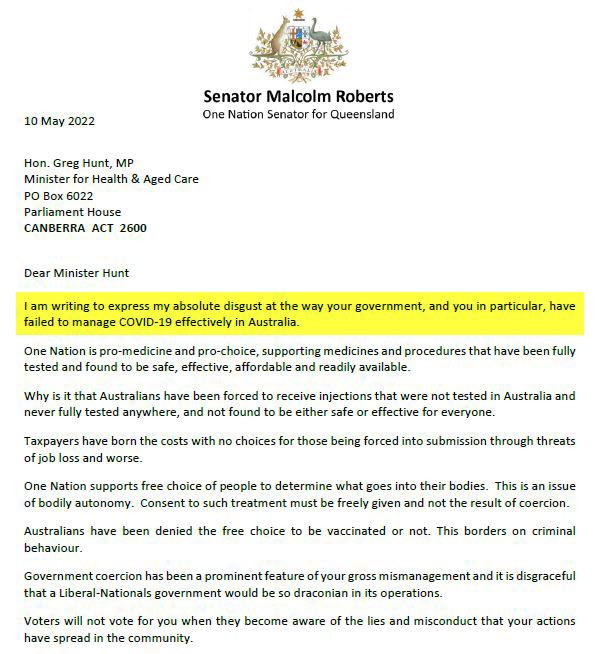
- FULL LETTER: May 13, 2022 LETTER TO GREG HUNT: HOW DARE YOU (external link) (PDF)
- FULL LETTER: Letter to Greg Hunt: How Dare You
John Larter, Former Paramedic “If AHPRA is given immunity by the Prime Minister for Health Professionals to speak out, this will be over”
- Fullscreen (Rumble) | Download (Telegram) | Download (Krystle Interview) (external links)
- Convoy Interviews & Speeches
Clinicians and researchers around the world have trialled various repurposed medicines and vitamins, zinc and nutritional supplements for Covid-19 with varying but often apparent success, particularly when used early and in combination. Suppression of such protocols that have long-term safety data by the TGA and AHPRA has deprived Australians of safe and possibly effective treatments.
As health care clinicians, we have the responsibility to gather Informed Consent from our patients who justifiably request this information, but we are hindered by AHPRA restrictions from discussing gene-based vaccine potential adverse effects, and the vital information for true Informed Consent is being censored by the TGA.
Suppression of early treatments for Covid-19 by the TGA and AHPRA
Off-patent or unpatentable and thus unprofitable treatments, used and researched for Covid19 by practitioners and researchers around the world, have been suppressed in Australia and other advanced economies, where a cynic could say a common factor is the potency of influence of big pharmaceutical companies.
The contrast of TGA and AHPRA suppression and alarmist statements on well-established medications and nutritional supplements, that have decades of safety data, with ATAGI and the TGA’s unfettered endorsement of experimental gene-based vaccines, that were rushed to market without many of the usual safety studies, and with only short-term phase 3 clinical trials that are now under a cloud of fraud and mismanagement allegations – could not be more obvious.
This letter is group signed under the auspices of the Covid Medical Network, Australia – that represents hundreds of clinicians and medical researchers who otherwise feel their careers are at risk if they sign openly. Several contributors to this letter are eminent in their fields. This in itself is an indictment of AHPRA and health employers, who are suppressing valid scientific discourse and the capacity of clinicians to assist their patients make Informed Consent or declination decisions. Others, not under AHPRA’s power, have signed openly.
In the aftermath, it is imperative that there be a major high level Judicial Inquiry to unravel the forces and reasons that led to the unhealthy overreach of official public health agency and governmental policies during this Covid-19 pandemic.
- Australian Medical Network – Open Letter to Atagi & TGA
- Covid Medical Network, Australia (external link)
To be fair to the medical community, this is not your fault. I have heard from countless doctors, nurses and patients that backroom bureaucrats—namely AHPRA and the TGA—are threatening medical staff with deregistration if they speak up about vaccine injuries. This needs to stop. This leads to the even more egregious act that people who have suffered an adverse reaction from the first dose of the vaccine are now required to get a second shot. What kind of cruel, inhumane act is this? Seriously, what has happened to common decency and human compassion? I note that Senator Keneally used the words ‘violent extremism’ and ‘violence’ a lot in her speech. But can I say that the threat of having to take a second vaccine if you’ve already had an adverse reaction from the first vaccine is violence in itself. It is intolerably cruel, and it is not something I intend to walk by.
- 22 Nov 2021 – Senator Gerard Rennick – Rumble | Facebook (external links)
- COVID-19 Vaccination Status (Prevention of Discrimination) Bill 2021: Bill | Hansard | Full Video (external links)
- [Rennick] COVID-19 Vaccination Status (Prevention of Discrimination) Bill
The government and media have placed doctors in an impossible position. The public have been told to speak to their doctors if they have concerns about the vaccine, but, due to the AHPRA’s gag orders, those doctors are not allowed to deviate from the current narrative for fear of losing their licence to practice. How can doctors possibly inform patients’ consent and overcome hesitancy when we’re gagged and have no long-term data? This is not informed consent. At best, it is manufactured consent; at worst, it is coercion.’
These are the same doctors who, when we were hit with COVID last year and there were no vaccinations, were on the front line, working in the hospitals beside the nurses. They put their lives on the line when we did not know what course this pandemic would actually take. Now they are treated like criminals. They can’t go into hospitals. In Rockhampton Hospital, there are shifts for which no doctor is available, because they won’t allow unvaccinated doctors to attend. We are on the verge of dividing our nation and people because of differences of opinion.
As the doctor said, they have been gagged. They are in fear of losing their licence or getting a heavy fine. This is not Australia—people being gagged this way. The whole debate on the issue has been stopped. The media cannot put across anyone who has a different opinion and wants to debate this. This is the only place we can do it—on the floor of parliament. Hence my stance with regards to this vaccination: people have a right to actually choose whether they want to have this vaccination or not.
- 22 Nov 2021 – Senator Pauline Hanson – Rumble | Facebook (external links)
- COVID-19 Vaccination Status (Prevention of Discrimination) Bill 2021: Bill | Hansard | Full Video (external links)
- [Hanson] COVID-19 Vaccination Status (Prevention of Discrimination) Bill
Barrister Raymond Broomhall
- 06:00 Vaccine is permanent – can’t be removed from the body – and the health effects are permanent as well. It’s forever. This also constitutes an assault or battery and a wounding.
- 06:29 Under criminal law, if valid consent is not obtained, it becomes an assault. If a doctor gives you injection and you haven’t given that doctor valid consent, then that doctor has assaulted you.
- 06:45 If a death occurs, that would then become a Homicide, if valid consent has not been attained.
- 07:00 In criminal law, valid consent means “Free, Voluntary Agreement, that is not Forced or Coerced“
- 07:15 Consent is invalid if there is extreme pressure or coercion.
- 07:20 AHPRA and it’s 15 National Health Practitioner boards promote and endorse ATAGI’s Australian Immunization Handbook.
- 07:50 Handbook is the approved guideline for Immunization providers. Valid consent must be obtained first, before administering a vaccine.
- 08:12 For the consent to be valid, it must be given voluntarily, free from undue pressure, coercion or manipulation.
- 08:30 A person does not give valid consent if he/she submits to a vaccination because of a threat of any kind, such as a “get the jab and you don’t have a job, can’t travel, can’t attend sporting or social events, can’t shop” etc.
- 08:50 The media also threats “Do the right thing and get vaccinated“, which implies if you don’t get vaccinated, you are doing the ‘wrong’ thing.
- 09:04 In effect, if anyone such as the media, politicians, employers, work colleagues, business owners, spruces the “Get Vaccinated – OR ELSE” narrative, it technically ostracizes people from society, and that’s discrimination.
- 09:28 If anyone succumbs to that pressure, where you got the jab but felt pressured to do so, that is technically ‘not consent’, which basically means “You have been assaulted”.
- 10:00 The doctor or immunization provider, should’ve asked you a question “Why are you here?” “What is the reason you are presenting for this vaccination?” Are you here to validly get protection from COVID-19, or are you here because you need to keep your job?
- 10:33 If the doctor realizes you have not technically approved under the valid consent principles, the he or she should refuse to give you the vaccination.
- YouTube | Rumble (external links)
- Laws against C19 Mandate [Australia] Barrister Raymond Broomhall
Why has AHPRA silenced health practitioners from raising concerns about what they call the experimental gene therapy (called Covid-19 vaccine); and why has AHPRA dismissed some seasoned health practitioners and threatened others with fines for raising genuine concerns that have been counter to AHPRA’s prescribed narrative?
Why is Remdesivir being prescribed by AHPRA in Australia and by the FDA in the US as part of the recommended treatment protocol whenever a previous trial with Remdesivir saw it kill so many people that it was withdrawn from the trial?
Aussie GP Speaking Out About C-19 Vaccines – Dr. Peter Johnston
Dr. Peter Johnston, a GP of 50 years, advised a patient to delay taking a covid vaccine until more was known about the long-term effects. As a result, APHRA accused him of spreading “Covid misinformation” and “undermining the National Vaccination Program“.
- Rumble (external link)
- Against Our Will [Australia & New Zealand]
- See also: Banned Australian GP speaks out (Nov 7 2021) – (Rumble) (external link)
AHPRA Silenced Australian Health Professionals
- Rumble (external link)
- The 9 March 2021 AHPRA Position Statement (external link)
Cat Got Your Tongue? Silenced by AHPRA
“GP can’t even answer my question on lockdowns. There are a handful more who will talk to me off camera, but not on camera for fear of disciplinary action by their regulator: AHPRA. Feeling ‘safer’ already from all that ugly ‘misinformation’ out there. Thanks AHPRA. I am reminded again how nice it is to be free of my career in medicine.”
- Cat Got Your Tongue? Silenced by AHPRA (YouTube | Rumble Mirror) (external links)
- The 9 March 2021 AHPRA Position Statement (external link)
- Dr Carolyne Bosak https://www.linkedin.com/in/dr-carolyn-bosak/ (external link)
- David Limbrick MP https://www.facebook.com/davidlimbrickldp (external link)
Dr Paul Oosterhouse & Dr Peter Johnston suspended
Dr. Paul Oosterhuis is an Australian anaesthetist with over thirty years experience, including in critical care and resuscitation. He has been brought before the Medical Board of NSW for posting information on social media regarding COVID-19. His posts related to early treatment and prophylaxis, PCR tests, and risk-benefit calculations regarding COVID-19 vaccination and lockdowns.
Dr Oosterhuis attended a Medical Board hearing on September 3rd, at which the Board suspended his registration. At his hearing, Dr Oosterhuis presented extensive evidence on the accuracy and defensibility of his social media posts, including their public interest value. The Board, however, declined to engage in any discussion regarding the evidence. Instead they enforced the ban on doctors contradicting the government, and suspended him without discussion.
- The Exiled Doctors Offer Shelter; Cafe Locked Out (Rumble | BitChute) (external link)
- Supporting Dr Paul Oosterhuis – Doctors for COVID Ethics (external link)
- NSW Medical Council media statement (external link) “The Medical Council has taken this action in order to protect the health and safety of the public and to maintain confidence in the medical profession. The Council has advised the suspension to the Australian Health Practitioner Regulation Agency (AHPRA) for recording on the public register of practitioners.”
Queensland Registered Nurse Carolyn Gaschk
Carolyn, a RN of 39 years, has witnessed nothing short of medical apartheid, high levels of coercion, gagging orders and injuries from shots across hospitals and medical facilities in southern QLD. This has lead her to taking a stand and speaking out and she’s here today, exclusively on The AJ Roberts Show to share the horrors that are now rife in QLD and across Australia.
- Registered Nurse Carolyn Gaschk: AHPRA Gag Orders Hiding Injuries and Deaths (Rumble) (external link)
AHPRA Silencing Doctors and Health Professionals – Tanya Davies MP
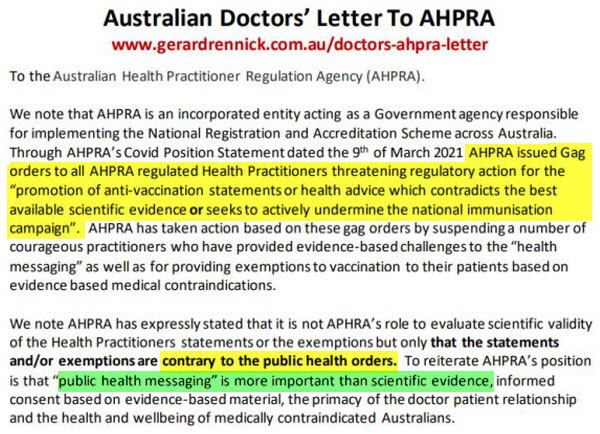
Back in March 2021, AHPRA, the Australian Regulating Body sent out letters telling all doctors to conform with federal governments vaccine rollout.
- Tanya Davies MP (Facebook | Website) (external links)
- The 9 March 2021 AHPRA Position Statement (external link)
- APHRA News March 9, 2021 Vaccination Statement (external link)
- Australia – The Australian Health Practitioner Regulation Agency Censored & Threatened Doctors (Rumble) (external link)
Dentist Dr Dan Hanson exposes AHPRA & their draconian demands
- Dentist Dr Dan Hanson exposes AHPRA & their draconian demands (Rumble) (external link)
Aussie Staff Specialist speaks out anonymously over vaccine injuries – Stephen Kelly
“I encourage any doctor or staff specialist with similar concerns to contact me skelly2063@icloud.com with similar concerns. Let’s send the good people at AHPRA a strong message that the truth must be told.”
- Aussie Staff Specialist speaks out anonymously over vaccine injuries (Rumble) (external link)
“Experts” Silenced by Policy
“Experts” Silenced by Government Policy including our own doctors who we’re told to go to for honest advice. Health professionals cannot voice their professional medical opinion if it doesn’t match the government’s medical opinion or interferes with the governments vaccination policy.
- We’re advised to “talk to your GP about the COVID-19 vaccines and what would be best for you in your circumstances”, but AHPRA (Australian Health Practitioner Regulation Agency) is telling our doctors that they will face regulatory action if they express any concerns that differs from the current government health advice.
- How can we trust that we are getting honest medical advice from health professionals who have a regulation agency threatening that their advice mustn’t contradict the government’s health advice or interfere with the government’s vaccination rollout under threat of their licence?
AHPRA Position Statements:
- https://www.ahpra.gov.au/News/2021-08-30-Joint-statement.aspx
- https://www.ahpra.gov.au/documents/default.aspx?record=WD21/30751&dbid=AP&chksum=zrOQ56xJaaLbasNxLDyqMA%3d%3d
- https://www.ahpra.gov.au/News/2021-03-09-vaccination-statement.aspx
- https://www.ahpra.gov.au/News/COVID-19/All-profession-information.aspx
This is kind of weird… as I was searching AHPRA’s midwifery board tonight, this came up in the search results on page one – weird date of 2005 came up next to their COVID-19 updates url – although it doesn’t show up in archives – earliest date I could find on 7 different archive sites I searched is 24 Mar 2020 (archive.org)…so probably nothing, just you know – when you see something like this, you wanna share it with someone :)
2017 – 2021
Evelyn Rae talks to Dr Jereth Kok, the Australian family doctor who was suspended for sharing articles from the Daily Wire and The Babylon Bee on his personal social media account.
- The Caldron Pool Show: Episode 10 – Dr Jereth Kok – Mar 14, 2022 (YouTube)
Website lists many issues with AHPRA from health practitioners from 2016-2021
- http://myahpra.com.au/news/ (external link)
- http://myahpra.com.au/parliamentary-enquiry/ (external link)
- AHPRA … a law unto itself (External Link)
- What can you do in 52 minutes? (External Link) AHPRA expect you to do a lot. If you don’t do what the Australian Health Practitioners Regulatory Authority (AHPRA) wants in 52 minutes, they publish a media statement that paints you in disparaging terms. It’s straight out intimidation.
National Conference 7th April 2017, Melbourne
Is AHPRA throwing rocks inside their glass house? Gary Fettke
2016
Charlie Teo Calls For Royal Commission
After hearing explosive claims about the medical profession from Dr Charlie Teo, we’re joined by Senator Nick Xenophon, who has been instrumental in the establishment of a Senate inquiry into this alleged bullying and harassment.
- Charlie Teo Calls For Royal Commission (YouTube) 17 Feb 2016
Medical complaints process in Australia
- Is bullying part of the culture of AHPRA? (external link) Is the culture of the Australian Health Practitioners Regulation Agency (AHPRA) to endorse bullying?
- Don’t Shoot the Messenger (external link) ‘Silencing’ of Gary, with the threat of deregistration should he continue to talk to patients, and the wider community, about the health benefits of reducing sugar and processed carbohydrates.
- “Enough is Enough” Dr Gary Fettke (external link) After 7 years of this inappropriate behaviour by both senior administration, and allied health practitioners, I say … enough is enough!
- AHPRA came after Gary for “providing nutrition advice to his patients”
- Breaking news … AHPRA drop all charges! (external link) Not only have they cleared Gary’s name of any wrong-doing, they have even apologised in writing!
- Community Affairs References Committee 22/11/2016 (Hansard | PDF) (external link)
- Parliament of Australia – Video – Nov 22, 2016 (external link)
National Conference 18th April 2016, Melbourne
Why AHPRA is more Dangerous than a Homicidal Client
- Fear-mongering starts at the top
- Threats from the PsyBA Chair
- Threats of deregistration
- Threats of fines from $5,000-$30,000
- Threats of being humiliated
- Threats of Registration fees
- Breeds fear & lack of trust
- They operate under a shroud of secrecy
- Destroy careers
- Why AHPRA is more Dangerous than a Homicidal Client YouTube
- Speaker: Sophie Henshaw
- See also: 2016 Conference Playlist (YouTube) – 16 Videos
The Institute of Clinical Psychologists Western Australia
It is our experience that the Psychology Boards and AHPRA have managed the administration of the Act inappropriately and that this has led to clinicians feeling bullied and harassed. The Boards and AHPRA themselves have engaged in bullying and harassment. A significant consequence is that AHPRA and the Boards divert practitioners from focusing on the clinical needs of patients and instead have to focus on avoiding the threat of litigation.
Summary:
- The Act and the system is punitive, draconian and provides the vehicle for the Boards and AHPRA to shame and humiliate health practitioners.
- The Act fails to deliver protection for the public because it provides for the Boards and AHPRA to focus on the narrow interests of the notifier as representative of public interests.
- The system is open to abuse because of the readiness of Board/ AHPRA to treat all complaints as serious and to accept complaints from anyone who has an agenda to abuse, bully or harass a health practitioner.
- The Act has permitted the Boards and AHPRA to believe they can ignore legal standards of proof and natural justice and to condone, by acceptance of notifications, the interference in Courts and tribunal processes, especially the Family Court.
- There is no provision in the Act for the Minister responsible to consult with the profession and this has allowed the Board and AHPRA to act without accountability, monitoring or feedback from the profession to the Minister.
- The system is also so complex, that the Minister responsible is unable to influence the Ministerial Council and therefore the policies of AHPRA and the Boards.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Royal Australian College of General Practitioners
- Overall, feedback from members indicates a perceived lack of balance in the system – where practitioners are subject to investigations that seemingly already assume guilt.
- The process, as it is currently administered, can be extremely stressful and onerous for medical practitioners. It involves a large time commitment from time-poor medical professionals and it can have significant reputational and professional consequences, regardless of whether the practitioner in question is at fault.
- It is perceived that the current complaints mechanism is more concerned with the prosecution of practitioners than protecting patient safety through remediation of the issues that lead to the complaint.
- The adversarial nature of the complaints mechanism can make practitioners question their clinical judgement, which could lead to different and possibly sub-standard management of a patient’s health.
- The stress experienced by practitioners resulting from a lengthy investigative process can also risk patient safety. It must be recognised that in order to put patient safety first, a fair and supportive complaints mechanism is essential.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Chiropractic Association of South Australia
- We would like to see a move to have complaints registered requiring the notifier to declare any conflict of interest to ensure the legitimacy of the complaint.
- This could be taken further by reviewing the number of complaints lodged by the same notifier over a period of time.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
National Institute of Integrative Medicine
- NIIM, as with the entire medical community, both integrative and conventional, aims for the fair treatment of all Practitioners under just and unbiased regulations and standards.
- The current complaints process does not accomplish this, nor does it allow for the practice of Integrative Medicine, and in many cases provides a total lack of natural justice to practitioners.
- Ensuring procedural fairness within the complaints processes, and a review process without bias, is critical for the wellbeing of clinicians and the industry.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Victorian Forensic Psychiatry Medicolegal Group
- Our experience is that AHPRA has little knowledge of the work psychiatric experts perform, no awareness of the hazards they face and no sense of proportion in responding to complaints about their work.
- AHPRA’s investigations look at complaints via a “health model” which is inappropriate where the parties are litigants and not patients or clients. Our clients are the courts, tribunals, lawyers and insurers that engage our services.
- We have lost trust in AHPRA as a body responsible for fairly mediating between IMEs and litigants.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Australian Medical Association
- AMA supports a compliance system which is transparent and accountable. It is vitally important that the profession retains the confidence of the public, and a transparent, easy-to-access complaints and disciplinary system is essential to achieve this goal.
- This system needs to be fair and uphold the principles of natural justice for all stakeholders.
- It is vital that the system shows a commitment to impartiality and due process.
- It is also vital that the wellbeing and state of mind of the practitioner be at the forefront of AHPRA’s considerations – particularly in investigations that are predicted to be long running.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Australian Psychological Society
- As outlined above, the rate of complaints against registered health practitioners, including psychologists, appears to be growing at a rate that is disproportionate when compared with the rate of workforce growth.
- However, the initial handling of complains against psychologists by AHPRA and the subsequent investigations by the Boards do not seem to be balanced and fair from the view of practitioners.
- The apparent heavy handed initial approach and delays in the investigation process, exacerbated by the lack of communication from the Boards to practitioners highlight an unnecessarily adversarial approach adopted by AHPRA and the National Boards.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Tasmanian Government
- I understand that, while covering various forms of bullying and harassment within the medical profession, the recent Senate inquiry into the medical complaints process in Australia (November 2016) drew attention to the misuse of the complaints process under the Health Practitioner National Law (the National Law) as a form of bullying and harassment.
- A number of examples were raised of practitioners whose careers and lives had been impacted by what they believe are vexatiously made complaints lodged by colleagues or competitors.
- Given the need to ensure the medical profession has a robust, transparent and respected complaints process to ensure public safety, the Tasmanian Government supports this new inquiry.
- This submission broadly responds to the six terms of reference of the Inquiry and highlights particular issues that may be taken into consideration.
- It is important to note that patient safety is paramount. However, the Australian Health Practitioner Regulation Agency (AHPRA) is equally bound by duty of care to the practitioner and the protection of professional integrity, and Tasmania supports natural justice and transparency in the complaints process.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Paddy Dewan: PhD MD MS MMedSc FRCS FRACS
- The principle problems with the current law governing AHPRA are:
- 1. AHPRA does not promote a collaborative collegiate patient centric mediation focused process of management of adverse events and complaint, thus enhancing a culture of conflict and fear.
- 2. The processes are legalistic and involve management by people with little or no clinical understanding.
- 3. There is no accountability of those involved in the management of the complaints.
- 4. The processes are not transparent and are not timely.
- 5. There are no rules of evidence for much of the process of handling complaints.
- 6. There is no appeal mechanism for the complainant.
- 7. AHPRA is part of the process of constructive dismissal.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Leong-Fook Ng, MA (Cantab), MB, BChir (Cantab), AM (Mal), FRCP Edin Registered General & Specialist Medical Practitioner (Medical Oncology)
- The fundamental doctrine of the separation of powers in the Commonwealth of Nations (the Westminster system, which includes Australia) must be operational in any real democracy.
- It appears that the joy of practicing as a health practitioner in Australia is now replaced by daily feelings of fear and angst amongst an increasing number of registrants.
- This impacts on the direct and indirect delivery of human services by both the public and private sectors.
- The basic requirements of acting according to natural law are unfortunately sometimes absent or capricious within the current operational jurisprudence of the Australian Health Practitioners Regulatory Agency (AHPRA) (and many of predecessor boards and their delegates) – being the “judge, jury and executioner” by way of National Law and some repealed legislation.
- This insidious malady, simply, is termed Sham Peer Review (SPR), subtly and strongly affected by the bond of ‘mateship’. It is also tempered with much influence from many ‘failed’ GMC UK policies and protocols.
- The recent Senate Report of 2016 on “Medical Complaints Process in Australia” (the Inquiry) highlighted many systemic and individual failures that were linked to bullying, coercion and harassment. Together with these was an endemic national culture of continuing crippling mendacity towards (and by) some from the professions, bureaucrats and also the public. The challenge is therefore a chronic systemic one.
- It appears that currently, the adverse regulation of health professions in Australia and management of non-registrants in healthcare are trending to an increasing number of cases, principally with fear-driven and swashbuckling non-evidence based approaches.
- This is unnecessarily oppressive, against the rule of law and stifles innovation, fairness and benefits to the public and the professions alike.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
DAVID McNICOL M.B., B.S., M.Sc., F.R.A.C.S., F.A.Orth.A Orthopaedic Surgeon
- It is my opinion that the current complaints system under the National Law, including the role of the Australian Health Practitioner Regulation Agency (AHPRA) and the National Boards is deeply flawed, due to the practice of the accepting anonymous complaints and acting on these complaints without careful investigation first.
- 2. This can lead to an immediate suspension of a doctor’s practice such that the practitioner is treated as “guilty until proven innocent”.
- This is DAVID McNICOL M.B., B.S., M.Sc., F.R.A.C.S., F.A.Orth.A Orthopaedic Surgeon Complaints mechanism administered under the Health Practitioner Regulation National Law Submission 39 a reversal of our system of justice, namely the “presumption of innocence”.
- 3. The investigation process of a complaint usually involves Medical Board staff and its lawyer seeking opinion from practitioners, from outside of the Board who are considered competent in the field of medicine under consideration. More than one opinion may be sought, leading to “doctor shopping”, to fit an opinion the Board lawyer[s] may have already pre-determined.
- Similarly, lawyers acting for the doctor do the same thing. This leads to an adversarial situation between the parties. This is an inappropriate way to arrive at a medically accurate assessment of a matter.
- 4. It is my opinion that the National Laws should be amended such that AHPRA and the State and Territory Medical Boards are required to involve the Colleges and Specialist bodies in the investigation of medical complaints.
- 5. The Colleges and Specialist bodies should be afforded legal protection in so doing.
- 6. Further it is my opinion that amended National Laws should require that a complainant’s name be made public, as in the Australian Courts, and that anonymous complaints should not be allowed.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
GARY FETTKE M.B.,B.S.,F.R.A.C.S.(Ortho), F.A.Orth.A. ORTHOPAEDIC SURGEON Tasmania
- The complaints process at present appears to be an advocacy role for the complainant as AHPRA’s guiding mandate is to protect the public, not work with the practitioners towards resolution. · AHPRA is staffed by people that are implementing the National Law yet do not have legal qualifications.
- There are health practitioners and lay people on the boards that are interpreting a National Law that has only just been developed, let alone tested. · The Medical Board seem to ‘make up the law as they go along’. My case is by way of example in:
- The Medical Board are acting on vexatious anonymous notifications without any demonstrated patient harm, nor actual complaint from patients or medical practitioners.
- The Medical Board are determining qualifications without deferring to the Australian Medical Council, relevant colleges or universities.
- The Medical Board are determining doctor patient relationships which have never been defined for media in all its forms.
- The Medical Board have made decisions based on hearsay, opinion and possibilities, without any factual content.
- Decisions have been made on perceptions of vested interests without definition nor audit. · There is no ability for the accused to have representation and an advocate throughout the investigation process.
- The health practitioner under investigation can only respond to decisions being made behind closed doors after findings have been determined. · The National Law and AHPRA have a process that has only been developed in the last 7 years and needs independent review.
- This is particularly applicable in the case of ‘Cautions’ that are non appealable, lifelong and without review.
- It is a complete travesty of justice to impose actions upon practitioners that have consequences on their careers, work and research opportunities without allowing an appeal process. Complaints mechanism administered under the Health Practitioner Regulation National Law Submission 54 3 · The current AHPRA process is ‘glacial’. I note submissions from AHPRA and other bodies commending themselves on bringing down ‘average’ times towards resolution.
- The Senate Inquiry has heard of many practitioners having years of investigation impacting their lives and their families. · Evidence is not collated in a timely fashion. · The investigators appear to be poorly qualified for the task of collation of evidence and presentation to Boards. The previous Senate Inquiry identified this as a concern.
- There are approximately 180 investigators assigned to AHPRA.
- Only 42 of 180 have a health background.
- Of those, 23 of 180 have a nursing background.
- Only 4 of the 180 have a medical background but their qualifications and experience was not defined by Mr Fletcher, AHPRA CEO in his November 2016 response to the Senate Inquiry.
- Over half of the ‘10000’ annual notifications to AHPRA involve medical practitioners yet there are only 4 people with potential qualifications to investigate these notifications with ‘insight’.
- There does not appear to be a clear ‘qualification’ required to be an investigator. o There does not appear to be a clear process of review of investigators.
- There does not appear to be a clear process to check that material supplied to the investigators makes its way to the Boards for consideration.
- By way of my own case, specific emails and responses have not been presented to the Medical Board. The Chairman of the Tasmanian Medical Board and the National AHPRA body have failed to acknowledge or respond to this as per recent correspondence from both parties.
- Evidence presented is not allowed to be assessed independently, that can then be scrutinised and challenged by the accused.
- The AHPRA process is not transparent.
- AHPRA and the National Law ‘hide’ behind the pretext of protecting the notifier and the ‘public’, but at what expense?
- ‘Evidence’ is withheld from the ‘accused’.
- Access to the ‘evidence’ is withheld despite numerous Freedom of Information requests. When something finally arrives, it is redacted to the point of ‘ridiculous’. · If AHPRA is challenged on their decisions, they retreat to a protectionist position. They have an immature response mechanism. By my own example:
- AHPRA’s finalisation of my investigation within hours of presenting to the last Senate Inquiry which I felt was intimidatory. Correspondence 5 November, 2016.
- AHPRA’s media release of 16 November, 2016 suggesting my obstruction yet not being able to respond in the time frame of 52 minutes
- he Senate Committee have correspondence regarding that from 20 November, 2016 and 9 February, 2017.
- The response of Mr Martin Fletcher, CEO AHPRA to the Senate Inquiry hearing on 5 November, 2016 in which he condones the intimidatory actions of his ‘team’.
- Complaints to the Health Ombudsman regarding AHPRA are referred back to AHPRA for internal review, incompletely addressed and then summarily dismissed.
- A direct meeting with the Chairman of the Tasmanian Medical Board on 6 December, 2016 was preceded with a ‘tantrum’. Prior to the meeting commencing he refused to enter the room whilst my wife was in attendance. This was accompanied by gesticulations, foot stamping, arm crossing, huffing and puffing and threatening to go home unless ‘she’ left the room. It was not a mature response by the head of the Tasmanian Medical Board. This was witnessed by others. Complaints mechanism administered under the Health Practitioner Regulation National Law Submission 54 4 o Following that meeting he requested further information regarding my case. Only many weeks later did he reply and incompletely. The difficult questions were left unattended and the initial inadequately. This example is common practice in my correspondence with AHPRA.
- Complaints to the Health Ombudsman about AHPRA are referred straight back to AHPRA for internal review. o In my case, that has happened twice and I continue with a ‘glacial’ response timeframe from AHPRA.
- AHPRA are the ‘Investigator, Judge, Jury and Executioner’ when it comes to notifications.
- The decisions are behind closed doors.
- The accused has no representation nor advocate in that environment.
- ‘Cautions’ are non-appealable, lifelong and without review process. o Even trying to find out how decisions are enforceable is difficult
- AHPRA and the Medical Boards are not respected by the health practitioner community.
- Every health practitioner that I communicate with has concerns of the AHPRA process. They do not trust it.
- The primary reasons are about process, transparency and accountability.
- Health professionals feel that once under investigation, you are ‘guilty until proven innocent’. That is an unhealthy environment.
- The AHPRA assessment process has not stood the test of time.
- It requires review.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
A/Prof. COLIN CM MOORE, MB,BS,FRCS,FRACS,FACCS,FAMLC Cosmetic & Paediatric Surgeon
My submission relates to two areas of concern:
(1) the lack of responsibility, at Law, on the part of public Servants/employees when they knowingly or unknowingly conduct their activities incompetently resulting in detriment to a Medical practitioner who is the subject of a complaint.
(2) In particular the failure of examining bodies (e.g. HCCC, professional standards Committees, etc.) to either be aware of or to ignore the existence of CONFLICTS OF INTEREST when seeking expert opinion(s), gathering evidence, &/or constituting Professional Standards or other committees.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Anne Malatt MBBS, MS, FRANZCO, FRACS
- A close friend killed himself last year, as a direct result, not of the complaint itself, but of the complaints process. Financially ruined, publicly humiliated, and personally devastated, when he could not take the strain any more, he took his own life, stating his innocence until the end.
- Of course, his death allowed people to think they were entitled to a presumption of guilt, but this presumption had been there from the beginning. Why is this? Why are doctors and other health professionals treated worse than common criminals?
- A criminal is regarded as innocent until proven guilty.
- They are entitled to a free and fair trial.
- They are entitled to free legal representation.
- They are compensated if found to be unjustly accused. Yet accused doctors are deemed guilty until proven innocent.
- We pay large sums of money in insurance for legal representation.
- If accused, rightly or wrongly, we are sometimes denied the right to continue to practise until the matter is settled, which can take years.
- There is no question of compensating us for loss of earnings, let alone loss of personal and professional reputation, if we are found innocent in the end.
- We are left to pick up the tatters of our lives with no support of any kind.
- And if we cannot, our family and friends are left with the devastation of our death.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Rachel Mascord BDS
Thus far AHPRA has resounding failed on all fronts. Promised efficiency has not been delivered to date, cost of memberships have risen, and the service offered by this overarching body has become starkly impersonal and indifferent to the needs of patients and practitioners alike. The chronic unresponsiveness of the organisation has failed to make greater protection for patients, and practitioners a reality.
What I would propose is a ground-up shift in approach based on the following principles:
- Natural justice must be afforded to the to the “accused” practitioner and the complainant. Both have a right to be heard fairly when investigations and hearings are conducted. There must be a presumption of innocence applied to the practitioner in question.
- Practitioners must be given fair and timely notice that a complaint has been made against them. There is simply no reason for investigations to be sprung upon practitioners. They are not criminals, they are not manufacturing drugs nor dealing in arms. There is no justification for the style of “raids” currently enacted by the Agency.
- The reason for the delays that draw out investigations must be identified as a matter of urgency and addressed. Any regulatory authority needs to be held accountable to its members, the Boards under its governance, the public and a government body that will regularly conduct audits on current investigations.
- Undertakings should not be imposed on practitioners without them receiving the appropriate advice they need to make such a decision.
- Investigations must be limited to the specifics of the complaint. If other faults are discovered co-incidental to the investigation they must be reported back to AHPRA for appropriate investigation, not swallowed up into the current investigation, creating confusion and uncertainty about what is actually being investigated.
- Transparency in investigations processes for complainants and defendants is essential. Information about the status of investigations must be made available to both complainants and defendants.
- Practitioners must be given access to the complainant’s treatment records and in a timely manner.
- Vexatious complaints and personal agendas must be promptly identified and addressed as such. There are clear red flags that arise when complaints are raised by people who have never utilised the service of a practitioner.
- There is a critical change in thinking called for. Adverse events and clinical errors are not malpractice, negligence, nor are they acts of malice. They must be seen and investigated for what they are, and not bundled in with acts of deliberate wrong-doing, reckless disregard for the well-being of others malicious harm. Without such a change in thinking, the current climate of fear of reprisal and defensiveness will prevail.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Yolande Lucire; PhD MBBS DPM FRANZCP
- The thrust of this submission is that the regulators would perform better (in accordance with the law, in accordance with their own codes of conduct, and in accordance with medical expertise) if staff of the regulators were made personally accountable for what they do.
- Malfeasance in public office is a personal tort.
- The regulators owe a duty of care to doctors, as doctors are members of the public.
- Regulators should be prepared to pay damages to doctors who have been inappropriately and improperly charged or convicted, without due process. Other courts and the Director of Public Prosecutions can have costs awarded against them, so medical courts should also be prepared to have costs awarded if they break the law, without the doctor needing expensive recourse to the Supreme Court of Appeal. This should be part of the service, and independent authority, as no one currently monitors this aspect of the regulators.
- The very notion that one is accountable would raise the standard within the regulators immeasurably. At the moment there are no checks and balances and no accountability, so the regulators are entirely out of control in a variety of ways.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Kevin G. Doyle
- I am concerned that this Senate Inquiry will be satisfied with itself in delivering, at best, recommendations for new laws, regulations and guidelines to “address” the obvious issues it has been made aware of by submissions previously received, although at this level of correction, we are still likely to see such laws, regulations and guidelines watered down sufficiently so as to not effectively challenge those “hidden” voices of power; those who benefit from the abuse of others – such abuse being the corrupt principle that the current status quo operates as and from and sadly, and further revealing of our lack of insight, most would consider that a great outcome for any Senate Inquiry.
- However, here I am asking the inquiry to go beyond just laws, regulations and recommendations.
- On offer is a choice to act upon a truth, a truth that once acknowledged, effectively and conclusively places this inquiry, its ToR and likely outcome as ineffectual if not counter-productive.
- As with this truth and many truths time and history has regrettably but necessarily been our relentless and often ruthless, yet loving teacher; however, have we listened and will we listen now?
- The introduction of new laws, regulations and guidelines have invariably been shown to be ineffectual even counter-productive as previously stated, unless we see concurrent culture change, only then do we witness true and thus lasting change.
- And Senators, this true principle, has yet again, been largely ignored by the inquiry by the ToR, yet I am clearly witness to its call from the many submissions to date. True change must begin from within, at the level of the individual and should be encouraged and supported in and by law.
- As this has yet to be addressed, we will thus witness the emergence of a greater level of cunning and deceit than, for example, the current enforcement methods applied within one of the status quo’s policing arms, namely AHPRA – who recently demonstrated the application of ruthless, sledge-hammer-like injustice in their inquisition of Dr Gary Fettke, all done contemptuously, purposefully and intently directly in front of you, the Senators, and the Inquiry’s eyes.
- AHPRA handed down their clearly corrupt judgement about Dr Fettke a mere two hours after his Senate presentation, exposing their complicit corruption, and glaringly revealing AHPRA’s arrogant positioning and untouchable attitude – no subtlety here in the message they were delivering to you Senators and, in fact, for us all to heed.
- This is what AHPRA has unfortunately become and what we all play a part in, with our equally complicit and, at times, “convenient” self-serving support of the status quo.
- This is the great ill society has become laced with, to its very foundations.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
David Charles Lindsay
- I am David Charles Lindsay. I was a Bulk-billing GP, a non-vocationally registered GP, at 403 George Street Sydney, working for 15+ years in Skin Cancer work.
- I had 50,000 patients on my files, and I had the best record in the Commonwealth for my line of work.
- I had Zero morbidity and Zero mortality.
- I was pursued for political reasons relentlessly by rival Doctors and the Disciplinary Authorities since 1991 (or earlier), for 20 years.
- As a Skin Cancer Doctor, I was de-registered in 2008, essentially for Rudeness, untidy handwriting, and accusing the Medical profession and the Medical Authorities of corruption, through staging of Complaints and abuses of Process.
- I should have been re-registered in 2011, but I am still waiting.
- After Dozens of Hearings and Tribunals I was De-registered for 3 years, in 2008.
- I have been unable to re-register as the NSW Court Psychiatrists have literally black-banned me, because I am still pleading my innocence and still alleging corruption.
- I am the most investigated Doctor in world history and most investigated citizen in the country, Doctor or non-Doctor.
- I was pursued before I even had a profile as a GP, and within 2 weeks of starting work as a GP in 1993.
- I had been targeted for removal from the Medical Profession, even before I commenced Private Practice.
- I received 100 staged and orchestrated false minor complaints, including a rigged Medicare Audit.
- They were in the form of Sting operations.
- Patients and Miscreant Doctors were recruited because of their Psychiatric vulnerability, and in particular, their Psychopathic personalities, thus making them the perfect ruthless and relentlessly pursuing Complainants.
- These false Complaints were overtly acted out, and meticulously and criminally planned.
- These Complaints all attempted a Clinical Integrity test, and a Rudeness allegation.
- Other accusations included: untidy hand writing, and apparent stubbornness (or is it recidivism) for pleading my innocence, and pointing the finger back in the direction of my False Accusers and the Medical Authorities, and accusing them of Corruption and Abuse of Process. Medicare Australia audited me, as well, (following pressure to do so, from the AMA, the HCCC, rival Doctors and three Specialist Colleges), every other year, for 20 years.
- They prosecuted me at the PSRC, also in 2008, but this Decision was set aside.
- I owed them $200 after 20 years of Audits!
- In 2008, I was de-registered at the Medical tribunal, for Rudeness and was labelled Delusional, because I accused the Medical and Disciplinary Authorities of corruption and abuses of Process, and the Patient and Doctor complainants of orchestrating false Complaints. (My Mother, Tallulah Glynne, a non-defendant, was also illegally tied into the 2008 Medical Tribunal Decision and labelled a co-conspirer and having a shared Delusional Impairment with myself, a rare if not impossible Clinical entity, indeed!).
- The Mental Illness label was used to Silence me, isolate me, discredit every future word spoken by me, and to Destroy me in the long term.
- I have no mental illness, I am innocent of all charges, and my story, although bizarre, is 100% true.
- My story is of hideous Psychiatric abuses by the Psychiatric elite, including: the recruitment of the psychiatrically vulnerable for sting operations, intentional psychiatric misdiagnosis of me, … and destruction of me, in the long term, through the use of Punitive Psychiatry to silence and exile me from the Medical profession and the general Community.
- This was all done to me, … simply because I was observant and outspoken, told the truth, was innocent from the start, and pleaded not guilty to all charges.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Simon Rosenbaum
- My own and others recent experience has highlighted a number of serious concerns.
- 1. The stated goal of the AHPRA/Medical Board is to protect patients, and not to punish providers. Yet by imposing extremely harsh conditions on practitioners, this can have the immediate effect of shutting the practice down, and causing great inconvenience, increased pain and suffering in some cases, and additional expenses to the patients of the practice, let alone to the doctor and employees. There seems to be no negotiation with the practitioner on how best to serve the interest of his/her patients once certain conditions are imposed. One recent example – a doctor was found guilty of a sexual advance on a patient. He was barred from consulting all patients, so his practice was effectively closed. He is appealing the judgement. Why was he not allowed to continue practicing with a chaperone present ? What measures has AHPRA taken to preserve continuity of care for the patients ? I venture they have done nothing at all. AHPRA is responsible for compromising patient care by not taking patient consequences into account when they impose conditions on practitioners.
- 2. The whole process has become increasingly adversarial. AHPRA and the Medical Boards retain top tier legal firms to press their cases. This means that a doctor must rely on his insurer to cover his expenses in defense. This increases the costs, complexity, and duration of actions, and should be reserved for only the most serious and urgent of concerns. A genuine inquisitorial approach to resolving concerns should be a necessary first step with any formal investigations. The practitioner could sit down with a medical expert member or delegate to the Board to explain events, not to a legal practitioner, or to an investigator that has no medical knowledge.
- 3. I believe that the number of investigators employed by AHPRA is close to 200, yet only a handful are medically qualified. This is a serious concern, because it means that decision making is delayed, not influenced by clinical expertise and experience, and errs on a very conservative side. The practitioner is guilty until proven innocent. 4. Issues of fairness. I think we all have the expectation that the law, and the implementation of the law should be fair. Where is the fairness when a doctor can be given just days to respond to a concern, that may have been sitting in a file somewhere within AHPRA for months, where AHPRA has no requirement to complete their investigations and resolution within a similar or determined timeframe ? During that time, conditions may have been imposed on a doctor that affect his practice financially, cause reputational damage, and impact patient care. There needs to be an automatic sunset clause on imposed conditions to force resolution within a fair and reasonable time frame. Where is the fairness when a doctor responds to a set of proposed conditions, item by item, only to have his response peremptorily ignored or dismissed without explanation ? Example : a doctor may have had a complication, or made a medical decision, resulting in a condition being imposed on his practice. Yet, over many years, his complication rate has been low, better than benchmarks, and when this was evidenced to AHPRA, had no effect on the imposition of conditions. There is no transparency in the decision making process. Where is the fairness when a doctor can only appeal an AHPRA decision via a civil appeals tribunal such as VCAT ? This introduces further delays and expenses. I believe that this is used as a tactic by AHPRA to deliberately frustrate responses by doctors. There needs to be a formal process by which a practitioner can appeal directly to AHPRA, within a timely fashion.
- 5. The power that AHPRA has is effectively unbridled, with inadequate checks and balances. The body should be subject to government, legal and health profession oversight, should be accountable to government for it’s expenses and performance, should be able to be sued in the event of poor decision making, and should have fixed terms of board member appointments.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Maxine Szramka MBBS (Hons 1) B Med Sc FRACP Consultant Rheumatologist
The current fear based, adversarial, condemning and punitive system based on the destruction of practitioner reputation is not working to keep the public safe. In contrast it is clearly demonstrated that it is putting the health and well-being of health care practitioners at risk, decreasing the quality of patient care and increasing the risk of medical errors and the cost of the delivery of health care in general. Heath care is being impaired on all levels with this current system.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
DR JANE BARKERI Academic Lead – General Practice University Centre for Rural Health
It is how AHPRA has interpreted and abused their power which is at question.
Surely the goal of a regulatory body is not to cause undue stress to health practitioners leading at times to bankruptcy, marriage failure, mental anguish, PTSD, inability to work effectively again and at worst suicide – even when found not guilty of the accusations. This system needs to be fair not only to patients but to health practitioners.
It is completely inappropriate that the body which controls registration is also the investigating body. This does not follow the rules of our legal system here in Australia. AHPRA acts as jury, prosecutor and sentencing judge.
- 2. Health practitioners should not be denied procedural fairness
- There should be open and excellent communication.
- Both parties should be fully and fairly represented.
- Both parties should have access to all available materials, the complaint and all relevant clinical information including the advice of experts.
- Those being investigated should be treated as though they are innocent until proven guilty, as our legal system decrees.
- The defending practitioner should have the right to nominate at least one of the expert witnesses to create an even playing field.
- 3. AHPRA itself should be accountable, and not immune to investigation or review.
- 4. The welfare of health practitioners must be given priority in this process
- Counselling with an independent therapist, to support the practitioner safely through the process, should be a mandatory part of the investigation Insurance should be available so that practitioners are financially protected and where appropriate, compensated.
- 5. The process should be completely confidential and not be made public until the final result is available. Practitioners should not be found guilty by the public or the media before investigations are complete. The present process of publicising investigations in process should be abandoned, as it is very damaging in what may be found to be an unfounded or vexatious complaint.
- 6. The whole process should be timely so that neither the patient nor the health practitioner suffers from a prolonged enquiry. Whilst a regulatory system is indeed warranted, the current system falls far short of protecting the public and the people who serve it, and indeed causes much harm to those who are doing their utmost to care for the members of our community.
- If we truly care about the health and wellbeing of the people in our community, we would do well to ensure that we are also caring for those entrusted with our own care.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Chandrika Barman MBBS
- The complaints procedure is unsatisfactory.
- If no patient has been harmed, then any complaint by colleagues should be investigated in great detail before any action is taken.
- Complaints by colleagues need to be taken with a great deal of caution.
- AHPRA accepts vexatious complaints and does not investigate either the complaint or the complainant. • AHPRA and the Health Care Complaints Commission appear incapable of recognising a completely fraudulent complaint.
- AHPRA or the Health Care Complaints Commission were incapable of recognising the difference between the term medical officer-psychiatry and psychiatrist.
- AHPRA or the Health Care Complaints Commission did not investigate a (completely false) complaint by a former colleague before it suspended a doctor’s registration. No patient had been harmed and there were no patient complaints
- AHPRA or the Health Care Complaints Commission did not investigate the truth or otherwise the report before passing a hearsay information to supervisors and peer reviewers.
- AHPRA or the Health Care Complaints Commission did not investigate a complaint before sending a falsely accused doctor, along with prejudicial and untrue information to a psychiatrist for examination.
- That is the regulator provided false and misleading information to a psychiatrist whose role was to investigate the accused doctors. They then engaged an incompetent psychiatrist who did not understand the meaning of the words she used and like the complainant, also conflated religious beliefs with delusions
- AHPRA takes no responsibility for its mistakes.
- It does not apologise.
- It does not publish an apology.
- It has no responsibility, there is no accountability.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Mr Joel Levin
The current AHPRA system does not address this balance. There are too many instance of people initiating investigations for a personal or professional vendetta, abusing public funds and requires and place an inordinate time demand on professionals to respond, adding great deal of stress and pressure on already taxing jobs. Just as there is a difference between someone acting professionally and someone misusing the power they have been given, it is my experience and opinion that the current complaints systems is currently wide open to similar misuse.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Dr Edwin Kruys & Susan Wall
It appears there is room to improve the complaints mechanism administered under the Health Practitioner Regulation National Law.
A recent senate submission by the Royal Australian College of General Practitioners reflected the feedback received via a member-wide consultation.
The feedback indicated a perceived lack of balance in the system whereby GPs were subject to highly stressful investigations that seemingly assumed guilt.
AHPRA’s most recent annual report notes that of the 2718 matters involving medical practitioners closed that year, 71.2% resulted in no further regulatory action.
But regardless of whether a doctor is at fault or not, the AHPRA complaints process can be stressful and onerous for doctors. It involves a large time commitment from time-poor medical professionals, can have significant reputational and professional consequences, and the stress experienced by doctors resulting from a lengthy investigative process has the potential to negatively influence patient care.
For that reason, it is important to ensure the complaints mechanism is balanced: ensuring patient safety while making sure that the process is fair and supportive of medical practitioners.
It seems that the current process is often more concerned with the prosecution of doctors than protecting patient safety. Remediation of the underlying issues that lead to the complaint does not appear to be a priority within the current system.
The RACGP submission raised concerns relating to the lack of support for doctors under the complaints mechanism. Support mechanisms are especially important for rural and remote doctors, as well as international medical graduates, who are often relatively more isolated and may have a smaller support network to call on.
Following feedback from members, the RACGP also raised concerns that AHPRA investigators and Medical Board members do not always have sufficient experience or knowledge of general practice to understand the nature or significance of a complaint.
In order for doctors to receive a fair investigation, all cases should be assessed by a medical practitioner with in-depth knowledge and relevant experience in the specialty concerned. The RACGP recommended that a wider pool of medical practitioners be sourced to ensure that cases are reviewed by doctors with an appropriate level of understanding of the relevant specialty.
Another key concern raised by RACGP members was that vexatious complaints were currently not filtered out, and the RACGP therefore recommended that a process be put in place to deter and penalise submission of vexatious complaints.
Vexatious complaints are often submitted by colleagues, rather than by patients. The submitting of complaints by colleagues was the focus of a 2016 senate inquiry into the medical complaints process in Australia. The final report from the previous inquiry is what prompted the current senate inquiry.
Communication and transparency were also identified as issues in the current system. The RACGP was informed of multiple scenarios where doctors involved in the complaints process did not receive information outlining the process or when to expect further communication. This uncertainty caused significant distress.
The RACGP recommended that a clearly defined process regarding the complaints mechanism should be developed and circulated to doctors after they received notification of a complaint, so they were aware of what to expect and when to expect communication.
The RACGP also reported that doctors were often contacted about the case by several AHPRA representatives. This was unsettling for the doctors involved, as there was a perceived lack of continuity of knowledge of the doctor’s circumstances. It would be beneficial for the complaints mechanism to strengthen the continuity of those contacting and managing each complaint.
Privacy issues were also raised. Specifically, members highlighted circumstances where details of a complaint, including findings of the investigation, were published online prior to completion of an appeals process.
Medical practices may be significantly affected by conditions that are published online and available for patients to access if it is done so prematurely. If the appeals process concludes that the practitioner is not at fault, the published conditions could have already jeopardised the reputation of the practice.
Another concern regarded the lack of security, with RACGP members noting that they have been asked to supply information via email. Members are concerned that they may be vulnerable to further prosecution for sharing patient information via an unsecure network.
The RACGP has made recommendations to the Senate committee on how to better manage sensitive information. Furthermore, a lack of promised timeliness of investigations came in for criticism. AHPRA states they aim to complete investigations within six months.
However, RACGP members reported instances where investigations had spanned several years. Timeliness is important for both for the safety of patients and the wellbeing of doctors who have been falsely accused, and their families.
The RACGP highlighted the necessity for the complaints mechanism to recognise that where practitioner wellbeing is affected, patient safety is at risk. In order to put patient safety first, a fair and supportive complaints mechanism is essential.
The RACGP offers a GP Support Program, a free service for members to access professional advice to help cope with life stressors.
Dr Edwin Kruys is a GP and Vice President of the RACGP. Susan Wall is a Policy and Project Coordinator in the PPI, Advocacy & Funding Unit at the RACGP.
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
Websites
Related Posts:
- Hidden Connections Within Australia’s Power Elites
- Senator Rennick “This is no longer about COVID” End the Mandates
- QLD Senator: Truth Bombs “We won’t let you get away with it”
- Australian Medical Network – Open Letter to Atagi & TGA
- Convoy Interviews & Speeches
- COVID Conflict$ of Interest Australia [Video]
- [Hanson] COVID-19 Vaccination Status (Prevention of Discrimination) Bill
- “Experts” Silenced By Policy
- C-19 Vaccines [Videos] Doctors & Nurses
- Covid Truth With Dr Judy Wilyman
- Aussie Health Workers On Jab Policies
- An Australian Engineer Speaks Out – The Many Mysteries Of Covid
- Laws Against C19 Mandate [Australia] Barrister Raymond Broomhall
- Senator Pauline Hanson Speech – on early treatments banned, vaccine long-term effects unknown – TGA adverse reactions – AHPRA gagged doctors, media censorship, clinical trials, blocking Australian-made vaccines and more.
- COVID Conflict$ Of Interest Australia [Video]
- Verifiable References For Aussies
- Against Our Will [Australia & New Zealand]
- Politics Block Lifesaving Medicines To COVID Patients
- “Trust The Science” Policy Vs Healthcare
- Preventing Severe Outcomes With Early Treatment Vs Government-Policy-Controlled Health Advice
- Revealing COVID – Another Retired Aussie GP “AHRPA Severely Threatening Doctors” & COVID Truths
- Pandemic Experts Left Out Of Covid Taskforces
- Tabletop Exercises
- Australian Parliament – Ivermectin
- AHPRA Profile Alan Morrison (External Link)
- AHPRA Member Profiles (external link)
- TGA – FOI 3093 (External Link)
- The AHPRA Inquisition Against Australian Health Professionals (External Link)
- Complaints mechanism administered under the Health Practitioner Regulation National Law (Dec 2016 – APH.gov.au) (External Link)
- Summary of Submissions Parliamentary enquiry into AHPRA (External Link)
- The 9 March 2021 AHPRA Position Statement (external link)
- Australian Doctors Speaking out against the Censorship & Policies https://covidmedicalnetwork.com/ (external link)
- Robert Clancy: Emeritus Professor of Pathology “A Sad and Shameful Day for Australian Medicine” – 13th September 2021
Government takes over Health Policies (external links)
(Government bureaucrats override your doctor)
- Ministerial directives and communiqués
- The Ministerial Council may issue Ahpra and National Boards with binding policy directions. Guidance about the National Scheme may also be issued. Policy Directions
- The Ministerial Council appoints members to the Ahpra Agency Management Committee and to the 15 National Boards and Ahpra publishes the announcements. Govt Appointments
- Health Ministers issue communiqués on National Scheme issues including proposed changes to the National Law. Additionally, the Queensland Health Minister issues co-regulatory funding determinations annually. Communiques
AHPRA Position Statements: (external links)
- https://www.ahpra.gov.au/News/2021-08-30-Joint-statement.aspx
- https://www.ahpra.gov.au/documents/default.aspx?record=WD21/30751&dbid=AP&chksum=zrOQ56xJaaLbasNxLDyqMA%3d%3d
- https://www.ahpra.gov.au/News/2021-03-09-vaccination-statement.aspx
- https://www.ahpra.gov.au/News/COVID-19/All-profession-information.aspx
Rewards & Experimental Injections Encouraged:
(Your health practitioners encouraged to become vaccine-salespeople)
- “Promotion of COVID-19 vaccinations: further information for healthcare practitioners and other advertisers” | (83.3 KB,PDF), (103 KB,DOCX)
Silencing Midwives & Nurses:

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:


Truth-seeker, ever-questioning, ever-learning, ever-researching, ever delving further and deeper, ever trying to 'figure it out'. This site is a legacy of sorts, a place to collect thoughts, notes, book summaries, & random points of interests.
DISCLAIMER: The information on this website is not medical science or medical advice. I do not have any medical training aside from my own research and interest in this area. The information I publish is not intended to diagnose, treat, cure or prevent any disease, disorder, pain, injury, deformity, or physical or mental condition. I just report my own results, understanding & research.
![[Book] 180° Unlearn The Lies You’ve Been Taught To Believe](https://pennybutler.com/wp-content/uploads/2023/05/feargusoconnor-180degrees.jpg)
![More Videos on TGA FOI 2389 [Dr. John Campbell]](https://pennybutler.com/wp-content/uploads/2023/03/tgafoi2389clancy-600x437.jpg)
