A question about the PCR Test?

My biggest concern is the wrong treatment in the COVID wards and the lack of early treatment for those infectious positive cases, and I have questions that I hope can be answered by someone in the field…
I wrote this as a question on my facebook account – August 28, 2021 – knowing that I have vaccinators, lab-techs, nurses, doctors and specialists as friends/family that may be able to answer.
I did not receive any responses, although that’s hardly surprising since most people who ‘believe’ that the PCR test is legitimate may not of ever questioned it and may think anything that says anything contrary is misinformed, thereby doesn’t register as something needing to be addressed.
I write here with the same question I had then, in the hopes that someone can explain it to me, and maybe even investigate it themselves a bit further so that we can get a further explanation.
Along with these questions, there is further research I did to try and truly understand: (Download)
I also have another blog post where I was collecting PCR Videos (the videos focus on a more public-friendly explanation of PCR tests, whereas this blog post is more explaining the other oddities I found that I have questions about, however, if you have absolutely no idea at all about the PCR tests, you should start on the videos page to get an idea on why we have questions in the first place):
- PCR Videos (Watch)
1.) There’s a published paper last year in the African Journal of Respiratory Medicine about Melbourne’s PCR test.
A CT of 40 for a “yes” is definitely excessive, should be drastically revised downwards, and CT measures should be recorded for every positive case. Detection higher than 30-35 cycles “should not be considered infectious/contagious”.
Sept 2020 – Cycle threshold as a measure of infectivity from Covid-19 PCR tests – Alberto Boretti – PDF (01)
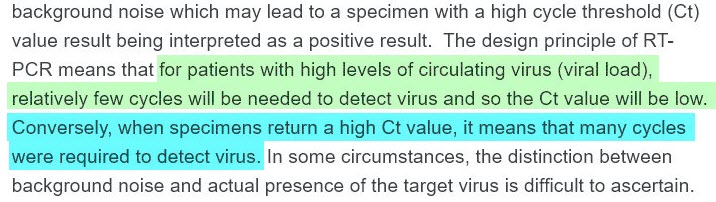
2.) WHO stated 2 months later (in Dec 2020) that a High-Ct result is unreliable and that positive cases detected at high ct’s would need to consider clinical signs and symptoms to determine whether it’s a true positive.
In a statement released on December 14, 2020 the World Health Organization admitted the PCR test used to diagnose COVID-19 is a hit and miss process with way too many false positives.
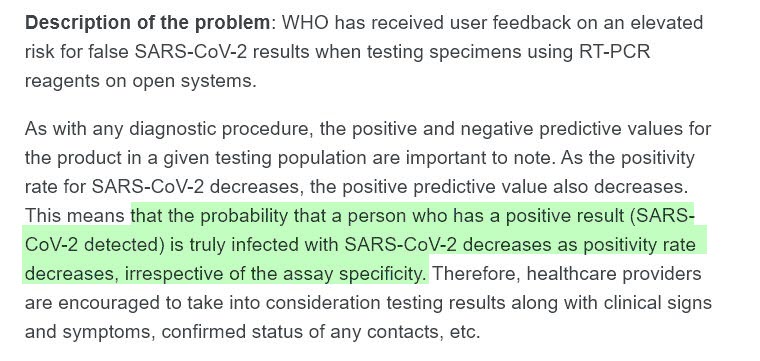
WHO Information Notice for IVD Users: Nucleic acid testing (NAT) technologies that use real-time polymerase chain reaction (RT-PCR) for detection of SARS-CoV-2 – 14 December 2020 (02)
3.) Fauci (Chief Medical Advisor to the US President) was interviewed saying that anything above 36 was dead nucleotides.
If you get a cycle threshold of 35 or more, that the chances of it being replication-competent are miniscule.
So that if somebody – and you know what we do – we have patients, and it’s very frustrating for the patients – as well as for the physicians – somebody comes in, and they repeat their PCR, and it’s like 37 cycle-threshold, but you never –
– you can almost never can culture virus from a 37 threshold cycle…so I think if somebody does come in with 37, 38, even 36. you gotta say y’know it’s just …it’s just dead nucleotides, period.”
Full Interview YouTube “This Week in Virology” (03) (3:54-5:45) (04)
4.) NSW Health Pathology States their Lab Equipment is set at CT 40-45.
NSW Health Pathology list their cut-off of threshold between 40-45 cycles. (05)
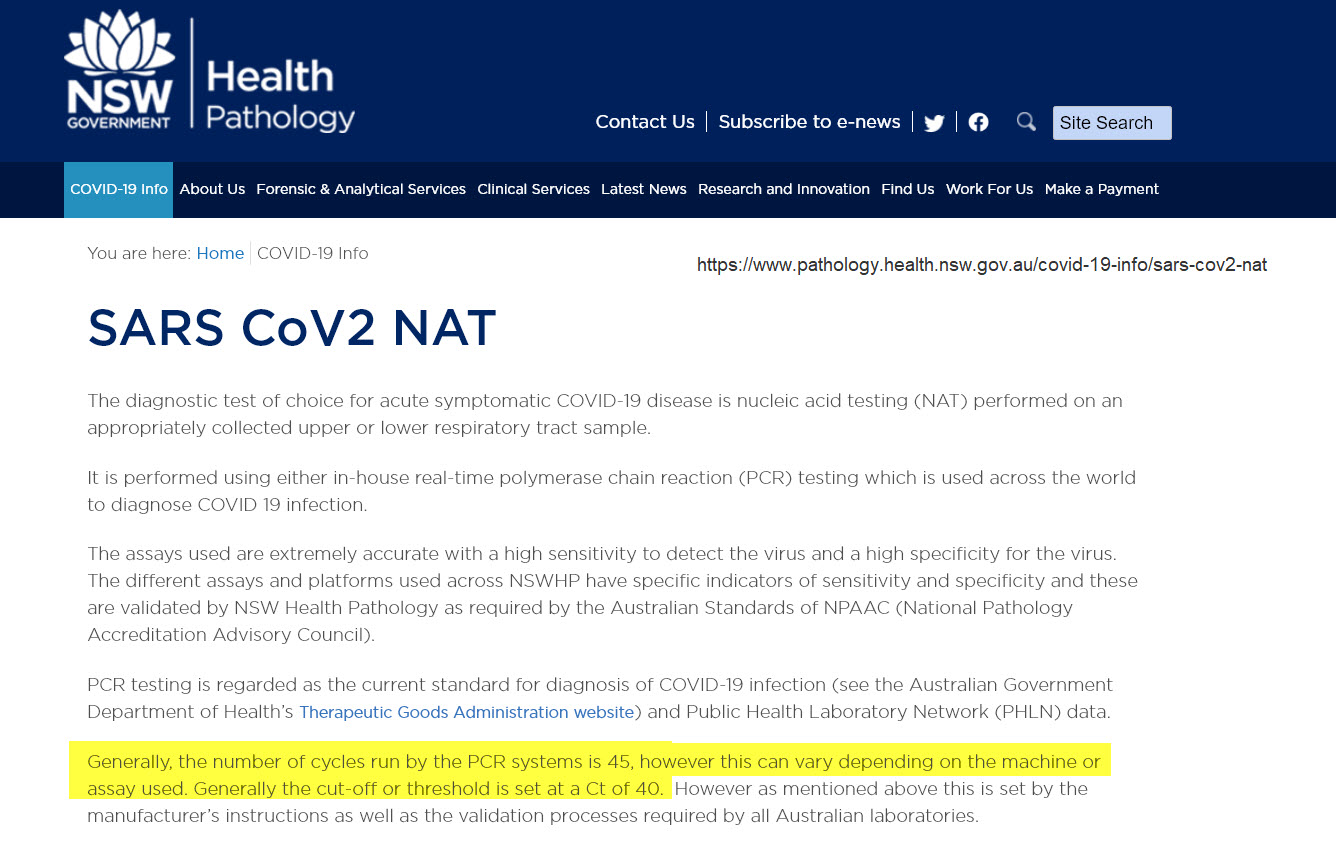
Generally, the number of cycles run by the PCR systems is 45, however this can vary depending on the machine or assay used. Generally the cut-off or threshold is set at a Ct of 40.
5.) Papers and lawsuits all over the world reporting that despite official health advice to the contrary, some governments are waging war on it’s own people – using the tests as a way to lockdown the nation.
Several published papers and lawsuits and even Dr Fauci says that anything above 36 was dead nucleotides – not infectious (not contagious). Beyond 34 cycles, your chance of a positive PCR test being a true positive shrinks to zero.
Various studies combined:
| Ct | Infectious/Not Infectious |
|---|---|
| <25 | “infectious” |
| 25-33.99 | “possibly infectious” |
| >34 | “not infectious” |

- RT-qPCR tests are quantitative tests. However, it appears that PCR testing is intentionally being used qualitatively, and cycle threshold values are being manipulated to increase or decrease case counts.
- Qualitative COVID RT-PCR tests are being used to do exactly what they are not calibrated to do, while confirmatory serologic viral load and antibody testing has been deemphasized.
- Qualitative COVID RT-PCR cannot determine whether a person is infectious and therefore should not be used to establish a diagnosis without the assistance of additional confirmatory lab testing.
Links to studies:
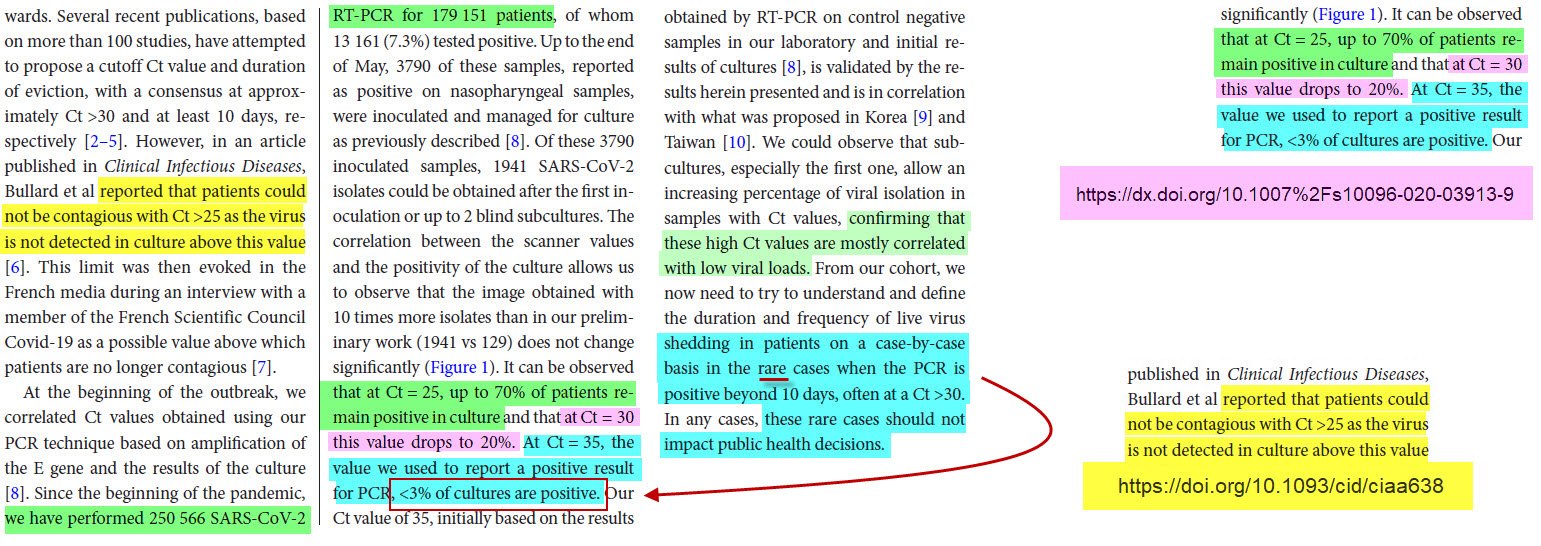
- “patients with Ct above 33–34 using our RT-PCR system are not contagious” (06)
- “A false positive test result can impede a correct diagnosis, delaying or depriving patients of appropriate treatment.” (07)
- “patients could not be contagious with CT >25” (08)
- “CT 25 infectious for up to 70%, CT 30 drops to 20% infectious, CT 35 less than 3% infectious” (09)
- …”there are numerous falsehoods, misconceptions, assumptions and exaggerated expectations with regards to capability, performance and usefulness of the technology” (10)
- 31 Mar 2020 … “to get 100% confirmed real positives, the PCR test must be run at 17 cycles. Above 17 cycles, accuracy drops dramatically.” (11)
- 3 Dec 2020 …”the odds of live virus culture reduced by approximately 33% for every one unit increase in CT” “Complete live viruses are necessary for transmission, not the fragments identified by PCR.” (12)
Links to lawsuits:
6.) PCR is NOT a test of “Infectiousness”
Apr 15, 2020 “PCR is not a test of infectiousness. Rather, the test detects trace amounts of viral genome sequence, which may be either live transmissible virus or irrelevant RNA fragments from previous infection“. (14)
Medically speaking, a “case” “SHOULD” refer to a sick person. It’s certainly “PROMOTED” by the Evil-Media as such, and generally “BELIEVED” or “PERCEIVED” by our standard TV-watchers. People think a “CASE” means “someone is SICK” – possibly “filling up our hospitals!”. Never should a “CASE” be ever referred to someone who is not sick, not infectious, never should a “CASE” be referred to a healthy person with no symptoms of illness!
Now all of a sudden, this well-established medical term, “case,” has been arbitrarily redefined to mean someone who tested positive for the presence of noninfectious viral RNA.
Drosten tests and tests recommended by the World Health Organization are set to a CT of 45. These excessively high CTs guarantee the appearance of widespread (pandemic) infection when infection rates are in fact low. (15)
Many – if not most – laboratories amplify the RNA collected far too many times, which results in healthy people testing “positive” for SARS-CoV-2 infection and being ordered to take off work and self-isolate for two weeks.
Let alone the alarming fact that those who “developed the PCR test for use in SARS-COV-2 detection, wrote THE paper that WHO used to recommend it as a valid test of detection to the world — with no viral isolate – just using the genetic sequence published online by Chinese scientists in January 2020., that it was published the very next day after it was submitted, and that scientists all around the world demanded the paper’s retraction pointing out all the fatal errors in it, stating that there was basis for reality in the paper at all ————- but the entire planet used this paper to start using PCR tests as a way to detect it? (16) (17)
A positive test, holds virtually no meaning whatsoever. Droston had setup his test to “guarantee” false positives. Anything over 24 cycles is completely unscientific. (18)
7.) A webinar with instructions to other labs from BGI Genomics.
At the end of a very long “webinar” to other labs – (BGI Genomics), he said… (19) (20) (21)
…”in addition to the control samples, we also used ‘known-clinical samples’ that were sources from another lab, and what we initially saw was a little disconcerting. We saw more not concordant results than we’d like to see. When we started investigating these results, what we came to find out was ‘in the samples that we recorded as positive, that the source-lab recorded as negative, we compared Ct values and found that…
… “the CT value the reference-lab had was below their cut-off – so they called it negative & BGI was able to pull that out at a higher sensitivity and determine positive sample”
8.) PCR Tests are incapable of differentiating between Flu A, Flu B, RSV (Respiratory syncytial virus)?
To get FDA EUA approval and for Quality Control, their equipment needs to test against a Positive and Negative control (regularly). These controls are also used to train new lab staff on detection. They (those in the webinar above) purchased their controls from a company called Zeptometrix. (A positive control that would test positive for “SARS-COV-2” and a negative control that would test negative for “SARS-COV-2”)
When you look at their sales pages for the controls, the 0.5ml controls are for Flu/RSV/SARS-CoV-2 – the one control… contains all 3.. Respiratory Syncytial Virus, Influenza (which we stopped tracking laboratory-confirmed cases of during the pandemic) and SARS-CoV-2
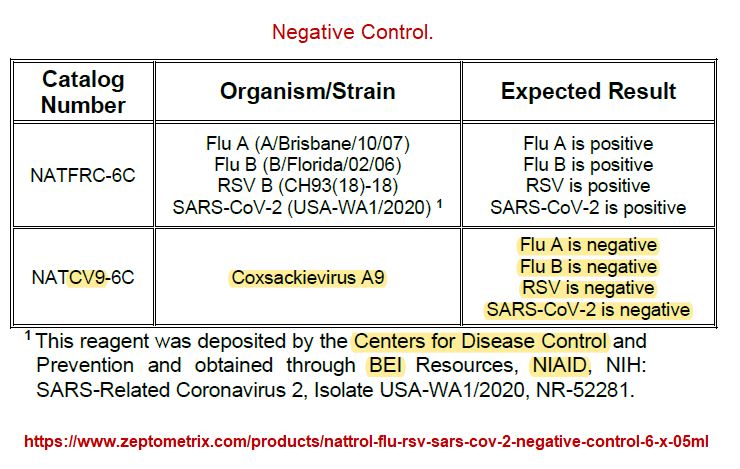
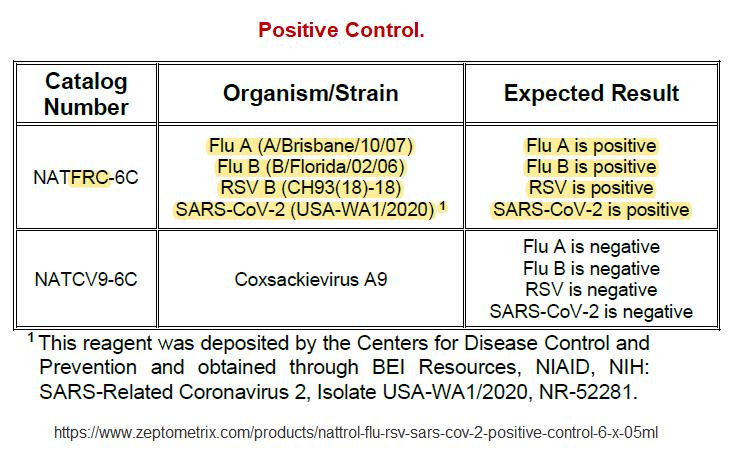
Zeptometrix Flu/RSV/SARS-CoV-2 Positive & Negative Controls (22)
9.) CDC, TGA, and every countries’ health tracking websites say they no longer track “laboratory-confirmed” Influenza (during the pandemic)
WHO/CDC/Australia & other countries require COVID-19 to be listed on the death certificate – regardless of how they died – if they were lab-confirmed or it was assumed to be a contributing factor in the death.
The latest (August 2021) CDC Flu weekly summary reports 17% of all deaths were due to pneumonia, influenza and COVID-19 but then said of those, only 4 were listed as influenza “indicating” the mortality is due to COVID-19.
(But unless I’m misunderstanding something – the tests themselves do not differentiate between 4 different respiratory diseases, and that hypothesis is validated by the fact that they do not track lab-confirmed cases of the other diseases)
I don’t have RSV stats (haven’t looked) but here are the Flu Stats:
- Lab-Confirmed Flu in Australia for 2017 was 248,112 (543 for pneumonia for interests sake)
- Lab-Confirmed Flu in Australia for 2018 was only 57825?
(I don’t understand why its almost 200,000 less than other years – anyone have an explanation for why that would be?) - Lab-Confirmed Flu in Australia for 2019 was 309,429
- Lab-Confirmed Flu in Australia for 2020 was 709 (health.gov.au dataset) or 436 (immunisationcoalition dataset)
So considering they aren’t tracking the flu due to “COVID-19”, there could be potentially at least 200,000-300,000+ Flu cases getting misdiagnosed and getting incorrectly treated with the new “COVID-19 Approved drugs” – (especially as the test is unable to differentiate & the symptoms are the same).
So regardless of all the ‘other impacts this has’… it’s an important question that I want to try and understand. (I don’t let things go until I completely understand them – and neither should any health professional, lab, or scientist worth a damn).
Flu Datasets Australia stop 3rd Jan 2020 (856 lab-confirmed 1st Jan – 3rd Jan 2020) (23))
Another flu dataset reports 436 lab-confirmed this year says “currently been suspended due to the COVID response” (24)
COVID Case numbers (25)
Immunisation Coalition Flu datasets (26)
You can download the datasets above from the official sites yourself, or you can download my research already collated: (In the “Cause of Death Reporting” folder – browse to:
Australia > 2017 (for the 2017 flu datasets)
Australia > HealthGovAu > Flu (for the 2008-2019 Flu datasets)
Australia > HealthGovAu > Pneumococcal (for the 2009-2019 Pneumonia datasets)
Australia > HealthGovAu > 2011-2021 Missing from Annual Reports.pdf (they updated this page in 2018 – but the only datasets available on the page were from 1997-2010)
10.) No Viable Virus Found in Positive Cases
The critique against PCR testing is further strengthened by a November 20, 2020, study in Nature Communications, which found no viable virus in PCR-positive cases. The study evaluated data from 9,865,404 residents of Wuhan, China, who had undergone PCR testing between May 14 and June 1, 2020.
A total of 300 tested positive but had no symptoms. Of the 34,424 people with a history of COVID-19, 107 tested positive a second time. Yet when they did virus cultures on these 407 individuals who had tested positive (either for the first or second time), no live virus was found.
How come we can accept a single virus sample – uploaded to a computer database – from China – and that is ‘trusted’ enough to determine the locking down of the entire planet, and the destroying of the world’s economy, the destruction of all communities, the censorship of all doctors and scientists, the creation of all the vaccines and the detection of the virus, but we ignore a study from the same city with almost 10 million samples?
Also, why the “Case Hysteria” – getting the public talking about “cases” when most “cases” are harmless?

Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China (27)
11.) “Please explain this to me”
My question for anyone that knows: This is the image I put together to ask experts to explain what it means.
(Please click image to open in new window to get the fullsize)

- In the middle of the image is the 2 controls that the labs use to calibrate their tests to ensure that it is ‘positive’ or ‘negative’.
- CDC, TGA, and all countries’ health tracking websites say they no longer track “laboratory-confirmed” Influenza (during the pandemic)
- WHO/CDC/Australia & other countries require “COVID-19” to be listed on the death certificate – regardless of how they died – if they were lab-confirmed or it was assumed to be a contributing factor in the death.
Download the entire folder of research in regards to Cause of Death Reporting. (28) - The latest CDC Flu weekly summary reports 17% of all deaths were due to pneumonia, influenza and “COVID-19” – but then said of those, only 4 were listed as influenza “indicating” the mortality is due to “COVID-19” – but the tests do not differentiate between 4 different respiratory diseases.
12.) My Questions:
1.) How are they able to tell when the tests themselves seem to be collaborated to test for Flu A, Flu B, RSV B, and “SARS-COV-2”?
2.) And what does that mean for hospitals/doctors – are they aware that they may be treating some patients as if they have “COVID-19” and therefore using ineffective treatments – when they could very well have one of the other respiratory diseases that they already know how to treat?
The treatments differ immensely depending on whether its COVID-19 or not – and what they are telling people when they have a positive test is “isolate for 14 days” – they are not giving them any treatment to “prevent” them worsening.
I was aghast when I looked up health.gov.au for ‘treatment’ to see what they recommended and it was a big fat “nothing – stay at home”. (29)
So for those who get their information outside of the television and criminal media outlets, can you explain how they are differentiating between the various diseases that turn up positive on the same test and present with the same symptoms?
Also very concerned that the very company that funded the Wuhan lab (which was under suspicion for creating “SARS-COV-2” virus/bioweapon) is the same company that supplies the “controls” for the testing (NIAID), the head of which is directing the show for all of us (Fauci) who is also invested in Moderna.
Fauci is director of NIAID (National Institute of Allergy and Infectious Diseases) (30)
Fauci’s NIAID “funded the 1st Moderna trial.” (31)
Moderna had up to $187 million in additional funding available from grants. (32)
Main Concern about this
Very concerned and suspicious at this point that the tests are being used as a weapon to lockdown healthy people and their contacts, and destroy the economy with a false pandemic declaration, and that the PCR tests are used:
- to approve certain experimental medicines, tests, equipment
- to keep the emergency state powers in the hands of the few and away from members being able to contest the things that are happening
- to quarantine healthy people
- to keep people in a constant state of fear of “air”
But my biggest concern and main question:
… for those who are educated in this area… is whether the doctors who are looking after people know that the test doesn’t differentiate between influenza and RSV and whether that is impacting those in their care?
Because if they are only testing for “COVID-19” and unable to tell the difference (symptoms are the same), that patients could be misdiagnosed and treated with these new experimental drugs & ventilators instead of what would work if they knew they were dealing with the flu or RSV.
So if you could explain the process (if you are in the industry – in a lab – a scientist in this field, a doctor working with these tests or seeing these patients) .. if you could please review my questions and let me know that would be much appreciated, thanks.
Also – not a single reference to which labs or “where” the sewerage tests are being performed in Victoria. Nothing – I cannot find a single source of information for this – if someone finds a source, please let me know because our gov on any page that I search trying to locate more information just says “we send to various organizations depending upon location”. No links, no references. That is not transparent enough for me when they are using it to force-test and force-quarantine various neighbourhoods calling them ‘hotspots’ with no way of validating this potential abuse of authority. Also – if you are someone that works in these places, can you do us a favour and test sewerage samples from 2017, 2018 and 2019 just for confirmation?
Other posts tagged PCR
- [UK] C19 Speeches – Pandemic Consequences
- Pfizer switched templates that could cause permanent genome changes to those injected & their offspring…[Senate Hearing]
- Bioengineered Clathrin Quantum Cognitive Sensors (ExQor / ExQori∆ / Xenqai)
- The Sequel to the Fall of the Cabal [Documentary]
- C19 Rapid Antigen Test Concerns
- FDA Rapid Covid-19 Tests Recall List
- [2f] Game is over: 5G – Directed Radiation & Predicting “Variants”
- BlueTRUTH [Parts-4&5] Testing “Unvaccinated” & References
- The UGLY truth about the Covid 19 lockdowns [PANDA 2021] (Part One)
- [ICIC] no new virus, no lab-leak, just a story & a bad test (Part 1 of 2)
- [ICIC] Australian Aboriginals Fight for Survival
- Basic PCR Questions to AI
- Advanced PCR Questions to ChatGPT [3/3]
- Advanced PCR Questions to ChatGPT [2/3]
- Advanced PCR Questions to ChatGPT [1/3]
- What is Going on in the World? [Summary]
- [Prof Nazar] C19 Vaccine-Bioweapon Genocide (paper & presentation)
- Reviewing c19=Bioweapon Patent evidence [Kingston]
- Convenient Deaths or Arrests (Whistleblowers)
- DNA Harvesting via PCR tests?

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:
 Aussies
Aussies Or Buy me a Coffee (PayPal)

References

![[RANT] What about now? Extraordinary level of denial — How do they still believe the narrative?](https://pennybutler.com/wp-content/uploads/2021/11/denial-kids-strokes.png)