Remdesivir—Run! Death is Near…

Remdesivir is the least effective, most expensive, and the most deadly treatment used during the pandemic. It’s “Eugenics”.
This post has videos and evidence to studies and case reports showing Remdesivir is deadly, and was the only “approved” treatment for COVID-19 in the US, and that it was likely used as a method to convince people they need the end-game: needle-rape.
- The first (2min) video is a teaser that gives you a brief rundown. (Dr Bryan Ardis)
- The second (9min) video is the summary of the evidence given at the Grand Jury (People’s Opinion Court). (Dr Bryan Ardis)
- The third is the full video (5hrs) presenting all the evidence, including screenshots, transcript, and links to the studies to the Grand Jury. (Dr Bryan Ardis)
- The fourth (2hrs) is the Truth for Health Foundation Conference hosted by LifeSite exposing the abuses and neglect of COVID patients in hospitals.
- There are many more to add when I have time, and I’ll continually add more videos to the last section.
Living document. First Published: April 13, 2022. Last Updated: May 9, 2022
Dr Bryan Ardis on Remdesivir
Pennsylvania Senate (2 min Clip)
“Remdesivir actually causes death of heart cells and is cardiotoxic and can lead to cardiac arrest. The only authorized drug to treat COVID-19 hospitalized Americans – even newborns and children – is Remdesivir. In New York State, 26.9% of Medicare-Aged Patients who received Fauci’s 5-Day Remdesivir protocol died“
- March 4, 2022 Expert Panel Discussion on COVID-19 and Medical Freedom | PENNSYLVANIA SENATE (01)
Grand-Jury (9 min Overview of Evidence)
“Remdesivir causes kidney failure as well as liver and heart damage”.
- Feb 14, 2022 Grand Jury (Day 3 – PCR Test) (02)
Grand Jury – Dr Bryan Ardis on Remdesivir – EVIDENCE
Referenced Evidence of Dr Bryan Ardis full testimony
The Ebola Trial: 2019
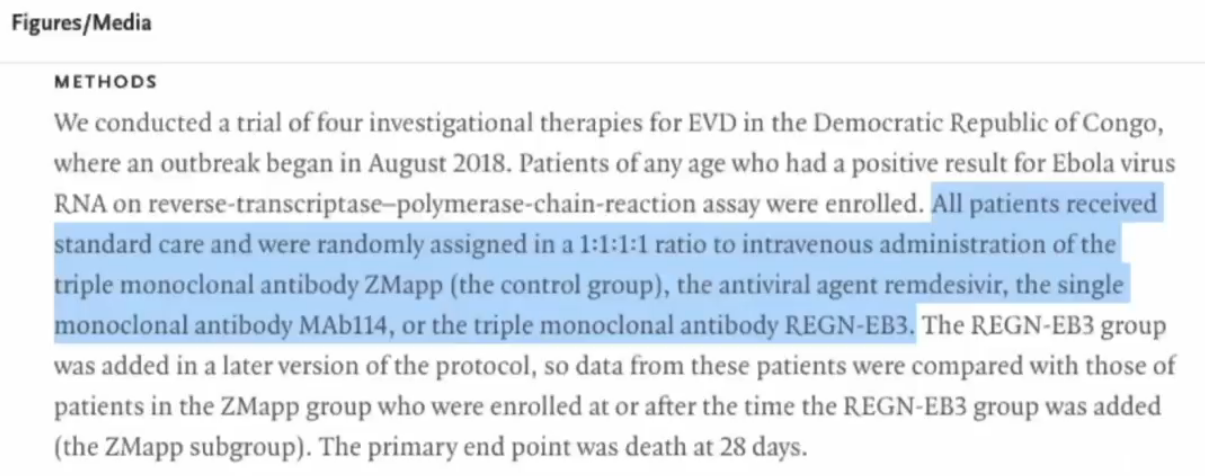
So, Anthony Fauci declared that in May of 2020 that there was an ebola trial in which remdesivir was found to be ‘safe and effective’ against the ebola virus. Did it? This is the actual trial, it still lives on the New England Journal of Medicine. (06)
You can see on the right-hand side of the page, it was published December 12, 2019. This study started in November of 2018 – and this is what they did.
They took four experimental drugs. All patients were given – you’ll see the three names ZMapp (which was a triple monoclonal antibody), you see an antiviral agent called remdesivir, a single monoclonal antibody called MAb114, and then a triple monoclonal antibody that the world knows about right now called regeneron (abbreviated REGN-EB3). This was the actual study. We’re going to go into four regions of Africa and we’re going to give four different drugs to ebola patients.
The conclusions – ‘right off the bat’, when you look at any study, they’ll give you a summary and then they’ll show you the conclusions – this is very nefarious and everyone needs to see this. ‘Right off the bat’, if you go in there right now, the conclusions were that Both MAb114 and REGN-EB3 were superior to ZMapp in reducing mortality from EVD.
Now I want to bring your attention to this. This is published on New England Journal of Medicine. Notice in the conclusion, they only list three drugs but in the study there were four drugs. It says, “Both MAb114 and REGN-EB3 were superior to ZMapp at reducing mortality from EVD”. But they said there was four drugs in the study. Interesting, right? They didn’t actually mention remdesivir.
Well, let’s find out why they didn’t want to show this on the conclusions at the top of the study.
All right, so just to bring everyone’s attention here. If you look down in the parentheses here, underneath “Conclusions”, you’ll see it’s funded by the National Institutes of Allergy Infectious Diseases; that’s who funded this entire study on ebola in Africa for the year 2018 to 2019.
Now, who’s the head of the National Institute of Allergy Infectious Diseases?
Just want to make sure for the world that it’s on record. You can see the director of the NIH NIAID department that funded the ebola trial is Dr Anthony Fauci. First statement is, “Dr Anthony Fauci was appointed director since 1984”, so he would have been the same director during this 2018-19 study. How did they screen these people for ebola? You’ve just listened to Dr Soňa. Now all the patients in the ebola trial, they used the PCR test to determine if they had ebola. Disgustingly, they actually allowed pregnant women using the PCR test to designate positive results for ebola.
They used pregnant women. Look at the last sentence, highlighted; even “neonates who were 7 days of age or younger” were included in this experimental drug trial in Africa, if the mother had documented positive for ebola. I find that pretty disgusting that an experimental drug trial you’re going to put in seven day old and younger kids – without symptoms – it just says, if the mother tested positive.
All right now, in the mortality section of this the study on ebola in Africa, on August 9, 2019 when 681 patients had been enrolled, the Data and Safety Monitoring Board conducted an interim analysis on data from 499 patients and, on the basis of two observations, in August 2019 they recommended terminating random assignment to ZMapp and remdesivir. So, the Safety Board solved two problems with ZMapp and remdesivir and terminated its use to be continued in this trial.
Well, what was so disturbing?
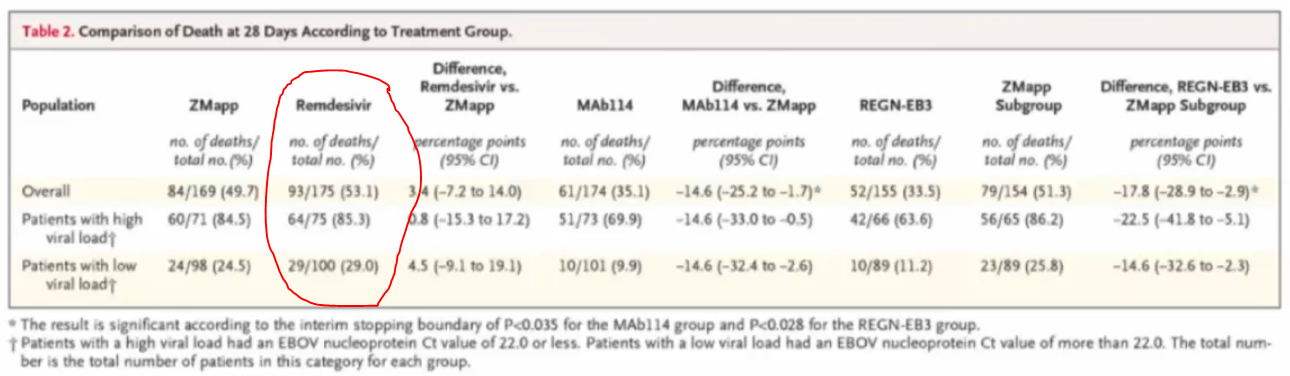
This is Table 2 from that actual study, to get the group’s eyes, here, and the audience’s eyes, here, and the Jury. Table 2, read the title, “Comparison of Death at 28 Days According to Treatment Group”. You have the population column on the left, then you’ll have four drugs listed: Z-Mapp, remdesivir, MAb114, regeneron is regn-eb3. The first statistic listed under each one of those is for mortality rate. What is the percentage of people given that drug in this trial that died?
ZMapp had a 49.7% death rate, you’ll see it in parentheses just below ZMapp, there in the highlighted area titled overall so Zmapp, everyone that got the drug 49.7% of them died.
Remdesivir had a death percentage of 53.1%. MAb114, 35.1% of everyone died. Regeneron, 33.5%. Based on this information, the Safety Board saw that remdesivir had the highest mortality rate and was the least effective in the trial and then decided to pull remdesivir and ZMapp from the trial.
Now, for the Jury, I would just like to present this to the Jury. If you were Anthony Fauci and you had this one study that you funded and you were going to be selecting one drug, and one drug only, to be the only drug pumped into all innocent American citizens with Covid-19, would any of you, any of you knowing what the Safety Board knew when they pulled the remdesivir, seeing it was the only drug that had a death rate of 53.1% or higher, which of these four drugs would you have chosen? And then I’d like you to ask yourself, why would Anthony Fauci have selected remdesivir when the Safety Board had its own concerns? Which one would you have picked if these are the only four drugs you had in the entire world to pick from? I would like to hope and think that you, as a health care administrator or overseeing a department for the entire country, would make a decision to pick one with the least mortality rate, like regeneron in this case.
Just to bring your attention here, this is at the end of the study, the National Institute of Allergy and Infectious Diseases. And then it lists the authors by abbreviation who actually contributed to the study. So, after I saw this ebola trial study, I knew Anthony Fauci was flat out lying – it was not proven safe and effective against the ebola virus (that’s what he said it did).
(Click images to open in lightbox)






Gilead trial: 2020
Then I wanted to know, well what did they find in the Gilead study? The Gilead study was done in March of 2020. You’ll see it was published in June 11th. This was their own studies. (07)
This was done from January – just so you know – the ebola trial published December of 2019. In that trial, remdesivir was pulled and found to be the least effective and the most deadly. Just a month later, January of 2020, Gilead is given the opportunity to do this study with remdesivir on Covid-19 patients. Now, the ebola trial was 28 days of drugging for those drugs per patient. And they found more people died from remdesivir than the other drugs.
In this trial in January of 2020. Gilead did something smart. They said, we’re only going to give 10 days of this drug to Covid-19 patients. Why? Because 28 days worth killed the most people in the trial that just finished a month earlier.
This is the published findings of Gilead. From their 10 days of remdesivir poisoning in Covid-19 patients.
23% had serious adverse events between days 5 and 10. “The most common serious adverse events – multiple organ failure, septic shock, acute kidney injury and hypotension.”
“Another 8%“ (below there) “discontinued remdesivir treatment prematurely.” They couldn’t even make it the full days, “one because of worsening pre-existing renal failure, one because of multiple organ failure” and two “needed to have kidney transplants as a result of the drug killing their kidneys”.
Now what was that being reported in the actual news? All I kept hearing was, ‘we’ve never seen a virus cause acute kidney injury‘, when, in fact, 31% of the people who got remdesivir for ten days were actually experiencing and reporting acute kidney failure from the Gilead trial just two months earlier!

France trial: 2020
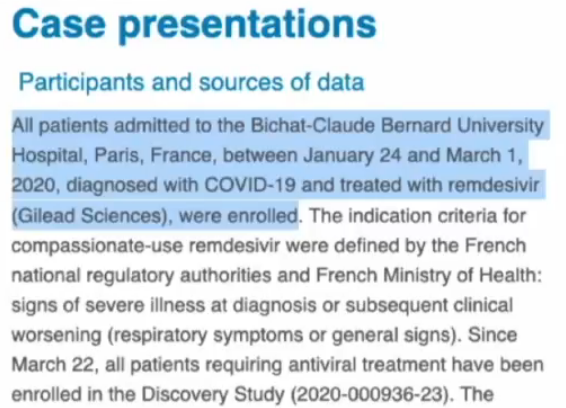
So, at the same time that ten days of remdesivir was getting pumped into the Gilead patients (53 Covid-19) patients, there was a study at the exact same time in France (except France took remdesivir in January to March of 2020). (08)
They only gave it to five people, five Covid-19 positive patients, including one from Wuhan, and they gave the drug for 14 days (this is in the beginning of 2020). What did they find? This is what they did.
So I just want to show the dates January 24th till March 1st. They were diagnosed with Covid-19 and treated with remdesivir from Gilead. This is who was enrolled there in Paris, France. What did they find?
They actually had set up a 14 day duration of treatment with remdesivir (highlighted part on the screen) from the study. Remdesivir was interrupted before the initial plan duration in four out of the five patients; two because of alanine amino transferase elevations – which is increased liver toxicity enzymes in the blood work abbreviated ‘ALT’ on most blood panels – they said this number liver toxicity was three to five times the normal range within those 14 days. So they pulled those two patients off the drug early.
And then continued and two because of renal failure requiring renal replacement. Now, for the Jury, renal means kidneys. So, two of the four who came off had to be taken off because their kidneys died requiring renal replacement. Before they were administered remdesivir, liver function and kidney function was tested and they evaluated them every day as they received these drugs.
Four out of the five patients had to come off early, two of the five had to have kidney transplants as a result. Only one lived through the whole 14 days. Two out of the five died as a result of the treatment of remdesivir. There’s a reason why France doesn’t have the death totals that we do. Now, that was conducted in and finalised in March of 2020.

WHO advices against Remdesivr 2020
Fast forward to November of 2020. Remdesivir, proclaimed by the World Health Organization – they determine and proclaim (read the highlighted part) –
“The antiviral remdesivir should not be used as treatment for hospitalized Covid-19 patients, the World Health Organization said Thursday, only a month after the Food and Drug Administration approved the drug to treat patients over age 12 who were hospitalised.”
October 22, 2020 was the date in which the FDA in America approved remdesivir as an FDA approved drug to treat Covid-19 patients. And the World Health Organization, just the next month (you’ll see the date on there, November 19th) said we do not recommend this based on all the data we’ve seen.
Gilead reported in this information and data collection by the World Health Organization, Gilead even stated remdesivir has potential side effects on the kidneys that they reported to European Medicines Agency. This is November of 2020.

Nature Medicine article 2020 – Gilead Conflict$
(Gilead makes Remdesivir)
For the jury and for the judge, I would like to present some information that’s become probably the most disturbing out of this entire two years of studying these hospital protocols.
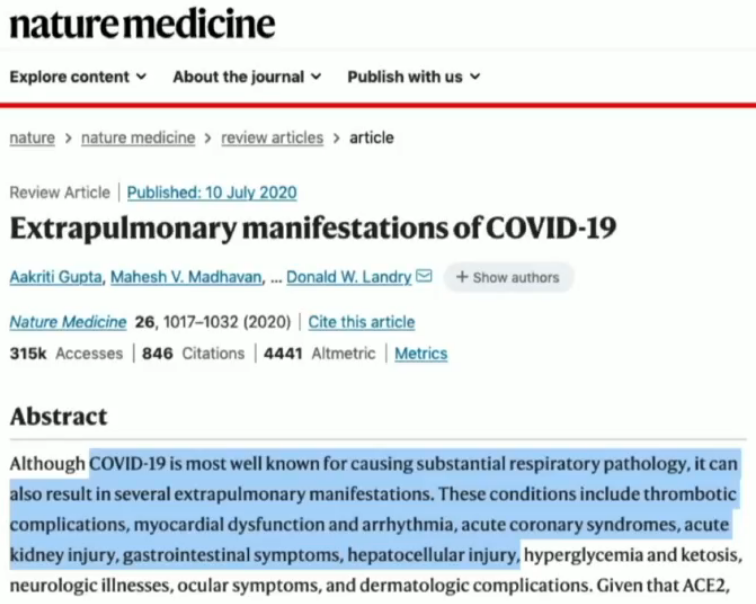
This is published in Nature Medicine July 10, 2020. I want you to read the beginning part of this abstract. This is two months after Anthony Fauci gets Gilead, the maker of remdesivir, to be the only pharmaceutical company awarded the only contract for the only drug to treat all Covid-19 hospitalised patients in the entire country of America. This summary, the title of this study is, “Extrapulmonary Manifestations of Covid-19”. (09)
This means, other than the lungs, what the virus does to the body, and causing disease of other organs. Let’s read the actual first sentence. Here, “Covid-19 is most well known for causing substantial respiratory pathology (or disease). It can also result in several extra pulmonary manifestations or disease processes outside the lungs. These conditions include thrombotic complications (that’s blood clotting disorders), myocardial dysfunction (heart disease) and arrhythmia acute coronary syndromes (which is strokes, heart attacks), acute kidney injury, gastrointestinal symptoms and hepatocellular injury (hepatocellular means liver toxicity).”
Now, when I got this actual article (remember, this is two months after Gilead Sciences is allowed to be the only drug manufacturer to provide a solution to all hospitalized patients for Covid-19), I already knew that the virus itself was not the primary cause of acute kidney injury, it was actually remdesivir, and the liver toxicity, as mentioned here.
But in Nature Medicine July of 2020, there’s this publication was made for the whole world to be able to see this new novel virus is causing these issues in the body, as doctors are treating it, so you know it’s actually the virus and nothing else.
Nature Medicine article 2020 reports
All right, so here’s what was reported in this study, “In China, the reported incidence of acute kidney injury in hospital patients with COVID range from 0.5% to 29% and it occurred with an average period of time within 7 to 14 days after being admitted in the hospital.”
So, between weeks one and two of the treatment is when acute kidney injury occurred. “But studies from the USA have reported much higher rates of acute kidney injury. In a study of nearly 5,500 patients admitted with Covid-19 in a New York City hospital system, acute kidney injury occurred in 37% with 14% of the patients requiring dialysis.”
Remember they all said ‘we don’t have enough dialysis machines here‘? And then read this, “About one-third were diagnosed with acute kidney injury within 24 hours of admission in the study.”
The only drug being used in that study in New York City hospital systems in March and April of 2020 was remdesivir. That’s the only thing different between what China was doing and what we were doing.
Nature Medicine article 2020, ethics — “I could not believe it”.
In the ethics declaration of this Nature Medicine publication about what the virus does for the entire world, as doctors are treating them around the world, we want you to recognize the virus SARS-CoV-2, (Covid-19) causes all these problems and on other organs in the body. Inside the ethics declarations where you you actually have to list those who are contributing to the data in the study, you have to disclose, do you maybe have a conflict of interest in being allowed to participate in contributing data? I put on the screen for the Jury, a woman named Joan, JMB, reports “an honorarium for participation on a grants review panel for Gilead Biosciences”. Why would someone on the payroll of Gilead be allowed to contribute, when they’re the only pharmaceutical company supplying the only drug to all Covid-19 hospitalised patients? Why would anyone on their payroll be allowed to contribute, to designate and define what’s the side effects of the virus you’re treating?
In fact, I’ll show you this is actually all the side effects, all of these here. These side effects that are listed here are actually side effects of remdesivir poisoning and we can prove it.

World Health Safety Database Review: 2021
All right, so remdesivir (this is April 2021), there’s actually a World Health Safety database review. (10)
What they want to compare is, around the world – which includes this audience – there are four major drugs being used to treat all Covid-19 patients. This is April 2021. They want to see if it’s true that the virus causing Covid-19 is causing an acute kidney injury in the majority of all people, a if it’s a side effect of the virus.
We’re going to look at the World Health Organization’s database and we’re going to look at and compare four drugs treating Covid-19 patients worldwide – remdesivir, hydroxychloroquine, lepinovar and a drug that’s a monoclonal antibody called tocillozumab. And this is what they found.
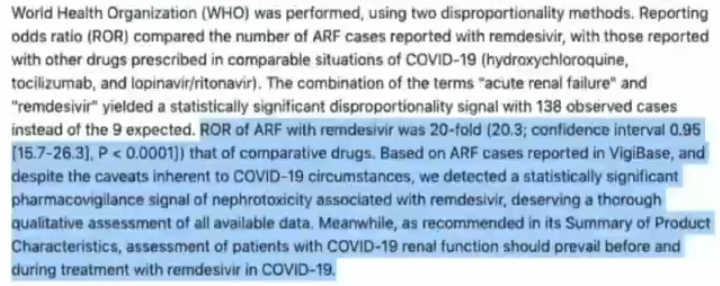
“Reporting odds ratio (ROR) compared the number of ARF cases reported with remdesivir, with those reported with other drugs prescribed in comparable situations of COVID-19 (hydroxychloroquine, tocilizumab, and lopinavir/ritonavir).”
This is important. The most important part of the entire thing is, they were prescribed these 4 drugs in comparable situations of COVID-19. Per the NatureMedicine publication (who said the ‘virus’ causes acute kidney injury.) They’re going to compare and see, “is it true?” Are all these covid positive patients around the world developing acute kidney failure, on an even-scale, and what did they find?
ROR of ARF with remdesivir was 20-fold (20.3; confidence interval 0.95 [15.7–26.3], P < 0.0001]) that of comparative drugs.
Twenty-fold! Not even close. Remdesivir IS known to cause acute kidney failure – absolutely.

Now, come full circle to October of 2021, just five months later after April, and there is a journal called the Cardiovascular Toxicology Journal, titled “Potential Cardiotoxic Effects of Remdesivir on Cardiovascular System”. (11)
Read at the bottom, “Remdesivir can also induce significant cytotoxic or cell toxic effects in cardiomyocytes (heart cells) that is considerably worse than chloroquine cardiotoxic effects. Remdesivir induced toxicity is due to its binding of mitochondria and the RNA polymerase.”
I need to reread this. In May of 2020 Anthony Fauci said “you cannot use chloroquine, you cannot use hydroxychloroquine with these Covid-19 patients because chloroquine was found to cause heart disease and death in Covid-19 treated patients, so, we’re only going to use remdesivir”.
In October 2021, you can see the date at the top, Cardiovascular Toxicology, first sentence (in the highlighted part), “Remdesivir can also induce significant cytotoxic effects and cardiomyocytes that is considerably worse than chloroquine cardiotoxic effects.”


Cardiotoxic effects comparison
This is a study from 2020 early on that Anthony Fauci would quote saying chloroquine and hydroxychloroquine increased the risk of death in Covid-19 patients. (12)
They said in this study all four regimens were also independently associated with an increased risk of new onset ventricular tachycardia or fibrillation. So, this study, they found there’s toxic heart effects due to chloroquine and hydroxychloroquine that’s increasing – read the title – the “risk of death in Covid-19”.
However, the Cardiovascular Toxicology Journal, just a few months ago, said remdesivir far worse causes cardiotoxic effects as compared to chloroquine as these studies proclaimed.

Nature Medicine (2020) said arrhythmias are the side effect of the virus,
arrhymthmic issues are a known side-effect of Remdesivir: 2021

All right, what are some of the other published cardiotoxic effects? If you start here (there in the highlighted part there), “there are some reports of sinus bradycardia, hypotension t-wave abnormalities, atrial fibrillation” (which is arrhythmic issues).
Remember Nature Medicine said arrhythmias are the side effect of the virus. It’s actually a known published side effect of the one and only drug getting pumped into your veins and a prolonged qt interval which is creating this lethargy and fatigue that everybody’s experiencing “and few cases of cardiac arrest and complete heart block following remdesivir infusion”.
Fauci knew that chloroquine was potential inhibitor 2005
Why is this significant? In 2005, Anthony Fauci knew that chloroquine was found to be a potent inhibitor of coronavirus SARS-CoV-1 back in 2005. Why? Why weren’t we publishing this, the conclusion of this study in 2005?
“Chloroquine, a relatively safe, effective and cheap drug used for treating many human diseases including malaria amoebiosis and human immunodeficiency virus (HIV), is effective in inhibiting the infection and spread of the SARS-COV-1 and cell culture”. We’ve known that for 15 years at this point.


NIH Table 2e COVID-19 Treatment Guidelines Charts Fraud 2021
This is important. The NIH has just updated these charts. This is actually titled “Table 2e” on nih.gov, last updated July 8, 2021. (13)
You’ll notice remdesivir is listed. Here you’ll see adverse events as the second column. I want everyone’s eyes to go to the fifth bullet point under adverse events for remdesevir. It actually states that the drug vehicle is abbreviated, “SBECD, which has been associated with renal and liver toxicity”. So we know it’s even published as a known side effect of the drug. On this chart dated July 2021 it was a broad titled characteristics, read the title, “Characteristics of Antiviral Agents that are approved or under evaluation for the treatment of Covid-19”. On this chart there was three drugs listed as either approved or evaluation by the NIH.
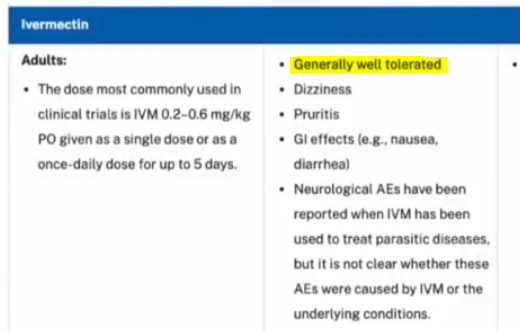
The second drug on that list was ivermectin, it gives you your doses of what to use in hospitalised patients. Very first bullet point in the second column under adverse events or side effects, “generally well tolerated”.
Now, I want to bring everyone’s attention to this, because they updated this chart in December. (14)
And they call it now Table 2f. Look at the date, last updated December 16, 2021 Right underneath the title, they list remdesivir. They list remdesivir as the only FDA approved drug now on this list.
But I want to bring your attention to ivermectin. You’ll see ivermectin right underneath. It says it’s “not approved” by the FDA and not recommended by the panel. And I want you to notice what they deleted underneath side effects of ivermectin – I’ve been pointing this out to legislators around the country and around the world.
They deleted the first one that said “generally well tolerated”. It’s the only one they removed. For reference, check this out. Table 2e: First bullet point, “generally well tolerated”. Now here, Table 2f, they removed it. They don’t want you to see it. They don’t want you to know it’s “generally well tolerated”.
All right, so I do want you know there’s, like, six or seven drugs on this chart. Now, in the NIH the actual drug remdesivir is the only one now titled in December of 2021, and still now as the only FDA approved drug to treat Covid-19. After it’s been published that it causes liver failure, acute kidney failure and now heart failure that we know and heart defects. (15)



CMS for Medicare add-on payments
Incentives to prescribe Remdesivir and to diagnose “COVID” positive case.
Disgustingly, the Centers for Medicare, Medicaid Services, here in the United States – Medicare covers all the elderly, Medicaid’s the impoverished and the disabled. But Medicare, right now, is actually offering – you’ll see the title – of the new Covid-19 treatments add-on payments per The Cares Act. This should disgust everybody in the Jury if it’s true that remdesivir causes acute kidney failure, liver failure and heart failure – it should disgust everyone to find out that CMS for Medicare is bribing all hospitals with a 20% bonus payout if they’ll just use remdesivir. And that bonus payout goes for the entire bill for Covid-19 treated patients. (16)
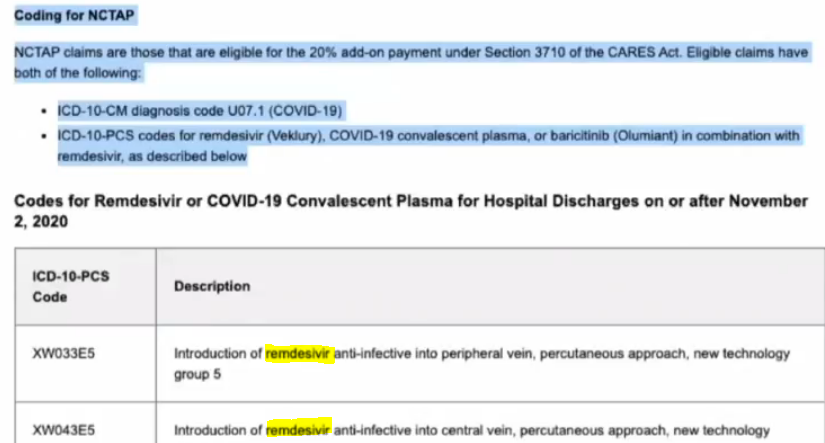
You’ll read here in the highlighted part, NCTAP claims are those that are eligible for the 20% add-on bonus payment under the Section 3710 of the Cares Act.
There’s two things they’re giving 20% bonuses for to all hospitals in America. For only Medicare age patients that’s 65 years and older – two bullet points
- – ICD-10-CM diagnosis code of U07.1 (that’s Covid-19 positive), that’s the diagnosis code they get a 20% bonus payout for.
- The second bullet point ICE-10-PCS (code for remdesivir).
- And then, below there, you’ll see the chart and they actually tell the hospitals, if you’ll just put down these two codes (those first two codes on the chart), we’ll give you a 20 % add-on bonus.
- If you just pick remdesivir, a drug known to be toxic and deadly (proven to be so).
Mortality results – Real time Analysis of Covid Treatments
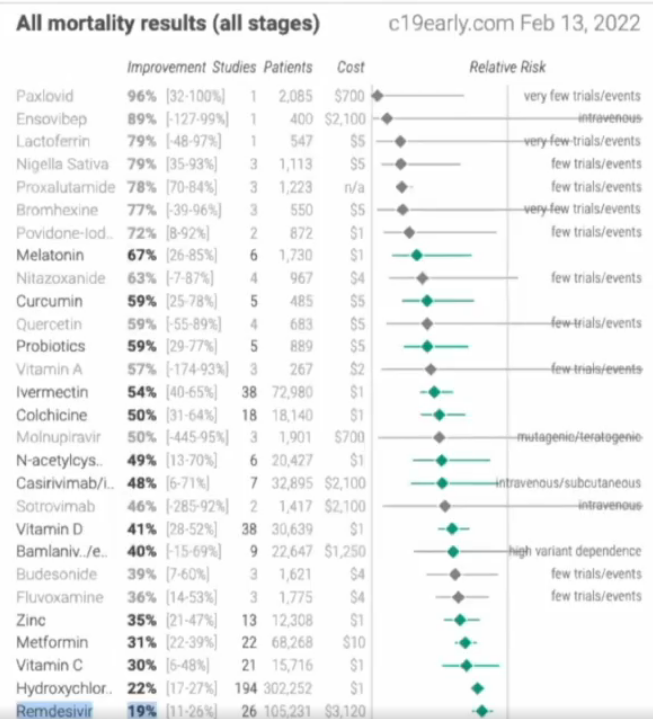
Now, I want to bring your attention to this. Why is Medicare continuing to bribe hospitals? Why? When, in fact… Look at this chart. Look at the date, top right. This is on c19early.com. (17) This is today, February 13th 2022. I want you to notice this is, the all mortality results. (18)
They take research studies from around the world being used to treat hospitalised Covid-19 patients and they want to know what of those drugs is producing the greatest rates of improvement and survivability. I want you to look at this chart. This is just as of this morning. Look at the bottom of the chart, that’s where remdesivir sits.
The second column is the improvement section, the percentages of all people in the research studies that are seeing improvements and not dying. Remdesivir is at 19% Improvement. And look at the amount of studies and the amount of patients in those studies. And then look at the cost of that failing drug, it’s over $3,100 per treatment which is a five-day treatment period. Almost everything above there has better results than remdesivir and this is worldwide studies.
My question is, why are we still supporting a drug two years later that is obviously failing worse than 30+ other products you can see here listed, which includes nutrients? You’ll see ivermectin on here at 54% success rate by itself that’s easily double remdesivir’s effectiveness at mortality, and improving mortality outcomes. Quercetin, you’ll see povidone iodines at 72% (and that’s a nasal wash and throat gargle that costs a dollar). Why are we promoting remdesivir? It’s the most expensive drug on this entire list and it’s one of the most failed.
FDA Statement Jan 24, 2022
In light of the most recent information and data available, today, the FDA revised the authorizations for two monoclonal antibody treatments – bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments.
The FDA has just updated as of January 24th, just a few weeks ago; they updated that because of Omicron variant, we are now discontinuing to allow REGEN-COV to be used in all clinics around the country, all states, all territories, all jurisdictions. And they actually claim that Omicron is not found to react to the treatments from those monoclonal antibodies that have been used and because of this data they’re now suspending its use. (19)
(I’m just showing you these things)
They list here in the highlighted part, “Importantly, there are several other therapies – Paxlovid, sotrovimab, remdesivir which is called Veklury, molnupiravir which is a Merck drug – “that are expected to work against the Omicron variant.” These are the only ones “that are authorised or approved to treat patients with mild to moderate Covid-19” in hospital, outside of hospitals actually “with Omicron variant”. And I want to bring your attention back to this.
They listed four drugs here; paxlovid, sotrovimab‘ veklury (remdesivir) and molnupiravir.

Out of everything on this chart I just showed you, paxlovid’s at the top. This is a drug created by Pfizer. it’s only had one study, two thousand patients, the average cost is $700. If you look at sotrovimab, it’s down right above vitamin D. You’ll see 41% and 46%, so sotrovimab is the second drug that they suggest – look at that, two studies with 1,400 cases, $2,100. Molnupiravir is four above sotrovimab. Molnupiravir’s at 55% success rate, three studies 1,900 people, $700 a pop. I want you to just recognize these are the most expensive drugs on here. Remdesivir was the fourth drug. There are so many other things that are cheaper and more effective and people should be referencing this.

Remdesivir EUA for Newborns & Kids!
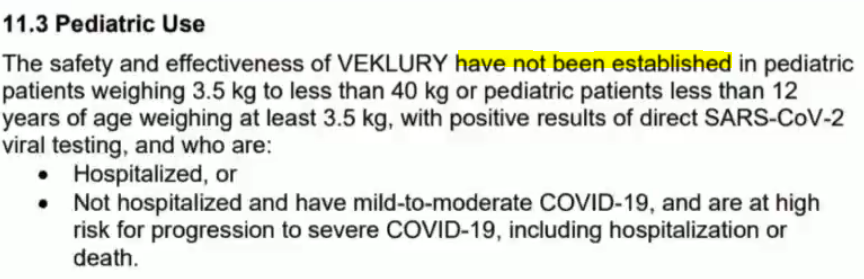
Three days before the FDA says, now you have to use remdesivir, sotrovimab, paxlovid and this other expensive drug, molnupiravir. Three days before that, the world needs to know this, the Jury needs to know it. This drug that causes acute kidney failure, liver failure and heart failure, it was just increased by the FDA January 21st. I’ll read this to you, “Fact Sheet for Health Care Providers (EUA) Emergency Use Authorization of Veklury (remdesivir) for the treatment of coronavirus Covid-19 in pediatric patients weighing 3.5 kilograms”. (20)
They are now authorising remdesivir to be pumped into the veins of all newborns weighing seven pounds or more and anyone in between. And they are PCR testing babies in hospitals as soon as they’re born looking to see if they test positive with a PCR test, and they will take them and inject them intravenously with remdesivir, a proven drug that kills heart cells called cardiomyocytes, liver failure and kidney failure.
I need to bring some things to the attention of the Jury, the Judge in the world n relationship to this document. It states “testing who are positive in hospitals or non-hospitals” (so this is in and out of hospitals).
EUA for pediatrics, parental rights
What every person needs to know is on this Emergency Use Authorisation by the FDA for pediatrics only, first bullet point here, “the parent giver/caregiver has the option to accept or refuse Veklury”. Please pay attention to that, all parents, you have the right to refuse per the EUA. Third bullet point, “Information on available alternative treatments and the risk of the benefits of those alternatives” have to be told by the health care professional. They have to tell you the alternative treatments that are available for your kid or your baby. I need to show you what’s in the document, though. Look at this.
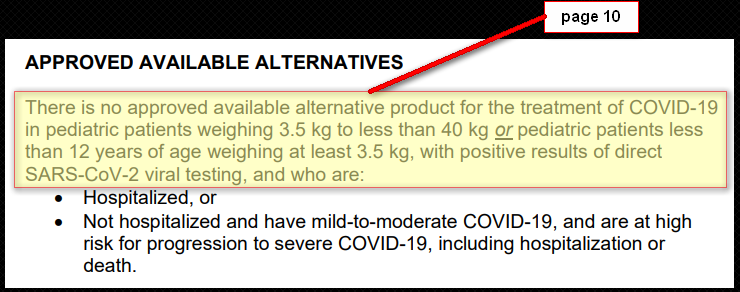
EUA for pediatrics, approved alternative treatments
It actually states, hold on let me show you, approved available alternatives. Look in the middle of the page, “Approved available alternatives”, this is on page 10 of the same document. Notice, it reads, “there is no approved available alternative product for the treatment of Covid-19 in pediatric patients”. Now wait a minute. They just said at third bullet point, here (previous slide), the doctors and healthcare providers have to provide information on available alternative treatments but later in the document they tell you there is no other ones that are approved only remdesivir.
Pediatrics, serious adverse events, reporting
It actually states here what they have to do if they ever give you remdesivir and there’s a side effect. Look at statement 7. It actually says, within 7 calendar days a healthcare provider has to actually publish on a US FDA form titled “3500 “all serious adverse events reported in babies receiving remdesivir“.
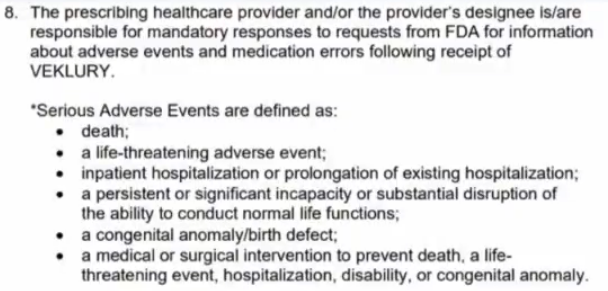
The world needs to know this, What’s the serious adverse events that could happen from remdesivir that they want you to report and are holding you liable for? Look here. Under number 8. Look at the asterisk.
Serious adverse events are defined as: death, a life-threatening adverse event, inpatient hospitalization or prolonging of existing hospitalization, a congenital anomaly or birth defect, a persistent or significant incapacity or substantial disruption of the ability to conduct normal life functions. Last bullet point, a medical or surgical intervention to prevent death, a life-threatening event.
All right, what else do you need to know? At the bottom of the screen, I want you guys to know why the EUA was given by the FDA for the use of remdesivir and babies.

It says here at the bottom “FDA has issued this EUA requested by Gilead, the maker of remdesivir, and based on their data submitted.” Okay, now I just want to bring something up here.
Why aren’t we having the other companies that make ivermectin, hydroxychloroquine, budesonide? They need to approach the FDA and just ask for an EUA to be able to be allowed because it looks like Gilead could do it. And based on their submitted data, I want to show you what the data is. It’s in this document. So, let’s look at the data that Gilead gave to the FDA to say, we can use this in pediatric patients now.
EUA pediatrics, “safety and effectiveness”
This is at 11.3. So, all the data for pediatric use. Look at this, “The safety and effectiveness of Veklury (remdesivir) have not been established in pediatric patients weighing 3.5 kilograms to less than 40 kilograms…for those who are either – bullet points – hospitalized or not hospitalized.”
So, I’d like to know what data the FDA had if it hasn’t been proven safe and effective with the pediatric patients. What data did Gilead give you? When, in fact, remdesivir is still proven to be the least effective and most dangerous of almost every one of these drugs that you see on this list?
I confer to the jury to find out why are they actually using this drug and continue to use this drug when, in fact, it is proven to cause more mortality, death and side effects than many more drugs.

Questions [3:06:49]
Viviane Fischer: Can you put up this slide again because I think in the footprint it said it’s being extrapolated or something from the information that we receive from studies from the adults. But, I mean, these were negative!
Ardis: Yeah, that’s right. Here, I’ll share it with you again. Yes. And what’s amazing to me is all the documentation about remdesivir and its failed publications and studies. (You can see it there on the screen.) “Use in this age group is based on extrapolation of pediatric efficacy from adequate and well-controlled studies in adults.”

And I am going to share something with you so the world can see this because they need to see it. This is the NIH Table 2f that I keep showing you. This was just updated December. This is table 2f. I just need to show you and scroll through this. It lists here remdesivir “approved” for the FDA treatment of Covid-19 hospitalized patients approved by the FDA. I’m going to scroll through here so you can see the list: interferon-alpha now is added to it, “not approved”; interferon-beta, “not approved”, interferon- lambda, “not approved” – come down here – ivermectin, “not approved”; ‘Nitazoxanide‘, “not approved” and then you come to the end.
There is no other drugs the NIH and Anthony Fauci are saying are allowed or approved for treatment, yet it discloses here that it causes acute renal failure.
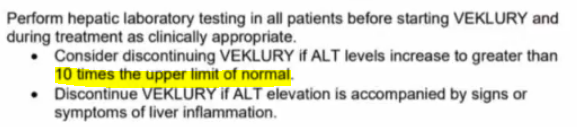
I don’t know if you noticed this here but this monitoring parameters remdesivir. It says, see the remdesivir section for information on using remdesivir for people with renal insufficiency. The monitoring parameters here lists that it’s okay that if we give someone remdesivir — in America you can actually watch the liver enzyme activities right here “ALT and ASD elevations”. They say, if you see ALT going up, (like they found in the French study; they pulled remdesivir when their liver ALT numbers went up three to five times normal) – they considered that toxic and deadly. Do you know what America and the NIH says is acceptable levels of ALT elevations? It’s in the remdesivir’s EUA. They allow your liver toxicity enzymes to go up ALT to 10 times the normal range. And for those who want to see it, I’ll show it to you because it’s in there and it’s disgusting to me.
EUA, protocols
Let’s show you. I have so much documentation here but I want to show you, just so you can see. The world needs to see. Why did it bother France and they pulled it off of there? “Increased risk” on page seven of the EUA for remdesivir “increased risk of transaminase elevations”. And I want you to go below to the bottom. Look at the first bullet point at the bottom. It says right above there, “Perform liver laboratory testing in all patients before starting remdesivir and during treatment.” First bullet point, “Consider discontinuing remdesivir if ALT levels increased to greater than 10 times the upper limit of normal.”
I would like to know why our NIH is okay with intoxicating a liver that the French scientist doctors pulled the drug knowing that it was deadly and toxic to inflame a liver, to have three to five times the normal levels of ALT, and they consider that life threatening. Why does our NIH, Anthony Fauci, and these protocols, why are they okay giving this drug to them?
And I need to show you the next one.
Risk, when combined
Right underneath this 10 times accepted level for ALT elevations liver toxicity, it actually states here …oh I need to show you. Hold up. I want to know what I was going to show you. Sorry about that. All right, so here you’ll see though, right below, it says “risk of reduced antiviral activity with co-administered chloroquine phosphate or hydroxychloroquine sulfate”. I need you to know.
Blood clotting
This says, these things are required.

Okay, number four, I showed you, you have to “Perform hepatic laboratory testing in all patients before starting VEKLURY”. Number five, you have to “Determine prothrombin time in all patients before starting vectoring and monitor during treatment, as clinically appropriate. I’m not sure if you guys know what prothrombin time is. But prothumbin time by definition, this is a clotting factor for blood. If prothrombin time is going up, it means it’s taking longer for your blood to clot and you will have internal bleeding. If prothrombin time is being shortened that means you’re actually getting blood clot issues.
So, this drug, they know, there’s two things you have to check:
- liver functions before and during treatment supposedly per the EUA;
- and you have to determine blood clotting time before and during treatment.
And I would like to know if everyone around the world is doing this at all. And I would demand that all health care professionals do this because this drug is proven to cause cardiovascular toxic effects including, as we showed you in the Nature Medicine, they said thrombotic events, blood clotting events occur due to the virus when in fact remember Gilead was allowed to participate in contributing their published side effects of the drug.
This drug needs to be taken out of circulation. There’s a lot more information on this drug. A lot more things that we have here but this drug by far, I believe, has been used just like the sedative drugs and this is not the only one. Remdesivir is targeting and killing the elderly. It’s complicating issues of liver failure, kidney failure and heart failure. But there are sedation drugs being used around the world, like midazolam, morphine – currently in America and in Canada. They’re using drugs like this to intubate these people who are being forced into having multiple organ failure – requiring them to go on to a Vent because they can’t breathe and these drugs are midazolam, morphine, lorazepam, precedex, and these drugs suppress the nervous system’s ability to control your ability to breathe. They are respiratory suppressive. They’re also known to paralyze the central nervous system and stop the heart from beating.
It is my opinion, they’re using these as euthanizing agents and protocols to speed up the actual death processes in hospitals and they’re targeting the elderly around the world and did from the beginning and we actually absolutely see that they are now targeting the young and now all people.
And, if of interest, if you don’t mind, can I show you one more thing. They are targeting the hearts of all these people with these drugs for sedation and with remdesivir as proven in those studies.
Circulation Journal, Warning
There’s one other thing I would love to show the world before it even comes up. I may not even be a part of it but, in the Circulation Journal. You just have to understand I believe there’s an asserted attack on heart muscle using remdesivir, using spike proteins and using the vaccines. You have to just see this because it goes right along the lines of what remdesivir has proven to do.
The American Heart Association publishes a journal called Circulation. In November 8th (you’ll see the date right there) they originally published November 8, 2021. It’s titled, “Mrna COVID Vaccines Dramatically Increase Endothelial Inflammation Markers and Acute Coronary Syndrome Risk as Measured by the Pulse Cardiac Test: A Warning.” (21)
And this is what they found at the bottom. “At the time of this report the changes to the heart persist for at least 2.5 months after the second dose of the mRNA vaccines. We conclude that the mRNA vaccines dramatically increase inflammation on the endothelium and the T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis blood clot disorders, cardiomyopathy and other vascular events following the vaccine. This is a warning.”
- Note, after this study went viral, the journal publication has been updated. They have revised the above sentence to read “In conclusion, the mRNA vacs numerically increase (but not statistically tested) the markers IL-16, Fas, and HGF, all markers previously described by others for denoting inflammation on the endothelium and T cell infiltration of cardiac muscle, in a consecutive series of a single clinic patient population receiving mRNA vaccines without a control group.” (22) (Most likely due to Dr Vernon Coleman, or maybe because Dr John Campbell’s review of it got almost 3million views, or any number of people – type the title into duckduckgo to see what I mean) (23) (24)
I only bring this up, not because this is the part of the Jury trial where you’re being taught about the side effects of the vaccines. You have to understand they are finding now that the targeted ingredients in the vaccines are targetting heart muscles. The blood clotting issues within the heart, they’re causing strokes, heart attacks and the American Heart Association is publishing this in November. This is a month after the Cardiovascular Toxicology Journal published that remdesivir causes thrombotic issues, cardiomyopathy and death of heart cells.
I believe there’s an onslaught attack to create targeted drug therapies or poisons that are directly targeting the heart of individuals, innocent people around the world and they are calling it Covid-19 deaths using falsified testing like PCR that we’ve already learned about here. And that is my argument. When in fact, we know there’s currently 150 studies promoting that natural immunity and, showing, that natural immunity, post infections from Covid – or anything else – are actually showing robust and longer-lasting immunity than any of the current vaccines that are actually being pushed on the public at large. (25) (26)

Fischer: Can I ask if there’s evidence of any conflict of interest or financial interests involved of maybe Fauci in what’s going on?
Ardis: Yeah. So, there was actually a meeting (I could pull it up) where Anthony Fauci met with 11 different people in discussing which drugs they were going to use as the solution for the pandemic and this was in March. Peter Breggin did a great job in his book of noting this in his book subtitled, “We Are The Prey”. Dr Peter Breggin. (27)

There was a meeting, Anthony Fauci and 17 other representatives, nine of them were in this meeting and they all worked at Gilead Sciences (wasn’t that amazing!) – that’s who he chose as his group of individuals to select remdesivir). So, that’s a great resource; 2000 citations in his book (about that).
I also will tell you there’s connections to Anthony Fauci/Gilead Sciences. I’ve already heard references in this trial today. People need to look into Gilead Sciences connections to Genome Tech and Roche and PacBio who’s creating these PCR tests. There’s a lot of collusion behind a lot of what they’ve done from the beginning and it’s been orchestrated since 2014-15. It’s a part of this entire “plandemic”. I will tell you, with Anthony Fauci and with the corporations that own Gilead (it’s primarily owned by corporations such as Vanguard and Blackrock), there’s tons of connections to Gilead, Anthony Fauci and others.
The selection, supporting the using of remdesivir, in my mind, is still to target the hearts, livers, kidneys of individuals. They know it’s toxic. The reason why I believe they are right now putting remdesivir (as of January 21st with the EUA as the only drug authorised to be pumped into the veins of all children – and there’s no other alternatives – is they need babies to start dying. Because February 15th was the FDA meeting that was supposed to be happening, to vote to give these vaccines to newborns, to five-year-olds, the Pfizer shots. So, I believe they are actually setting this up, one step after another, in lockstep, to create more carnage (more death, more trauma), blaming it on a virus that, like this Omicron variant that is almost the common cold (and I would argue it actually is the common cold, personally). But they want to actually project that this is deadly even in pediatric demographics, so they can sell parents/grandparents that they need to get the vaccines as well. And that’s the only reason why they would do it. I can’t find any other reason why you would do it.
Even when I showed you the mortality results document from c19early.com, updated daily, you see remdesivir’s effectiveness at actually preserving the lives of people with Covid-19. It’s 19% from research studies worldwide; two years later, 19% percent. I would like to ask the Jury why are we still promoting this one and only drug?
It’s now actually authorised to be used in all nursing homes in America, by the way, outside of hospitals as of the January 24th (FDA update). So, just like midazolam/morphine being used in the UK to kill innocent elderly people there – and call it Covid-19 – they are now setting the stage to do it here with a drug called remdesivir. And with the published documentation I gave you, there’s no reason on the planet, I would consider it safe to be given to the elderly when, in fact, right now February 13, 2022, there’s less than 1% of the entire world that’s gotten this virus and been infected with it. Who has died? Less than 1%!
In the state of New York, we pulled CMS data with Attorney Thomas Renz and his CMS whistleblowers. The entire state of New York alone, every Medicare patient who has received five days of remdesivir treatment for Covid-19 in the state of New York, the entire mortality rate is 26.9% of all of them died. When I say they’re targeting the elderly, they know these drugs are going to be toxic to them. And so, anyway, these numbers are disturbing. Why would you use a drug that’s failed to this extent, continued on two years later, unless there’s an attempt and a plan of genocide, to then sell the massive amounts of public around the world that you need our vaccines which are obviously failing? And you’ll go to that further into the trial.
More Remdesivir Evidence
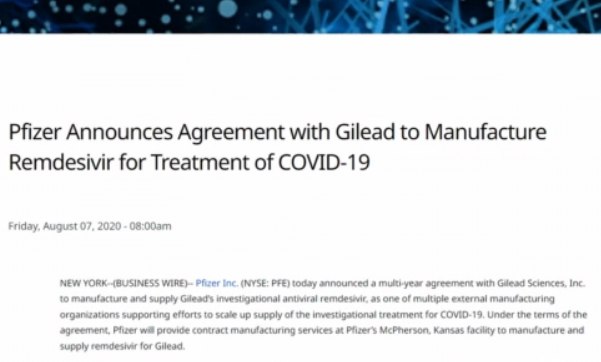
Pfizer Press Release, August 7, 2020 (28)
Pfizer Inc. (NYSE: PFE) today announced a multi-year agreement with Gilead Sciences, Inc. to manufacture and supply Gilead’s investigational antiviral remdesivir, as one of multiple external manufacturing organizations supporting efforts to scale up supply of the investigational treatment for COVID-19. Under the terms of the agreement, Pfizer will provide contract manufacturing services at Pfizer’s McPherson, Kansas facility to manufacture and supply remdesivir for Gilead.
https://www.pfizer.com/news/press-release/press-release-detail/pfizer-announces-agreement-gilead-manufacture-remdesivir

See also: Pfizer Whistleblowers
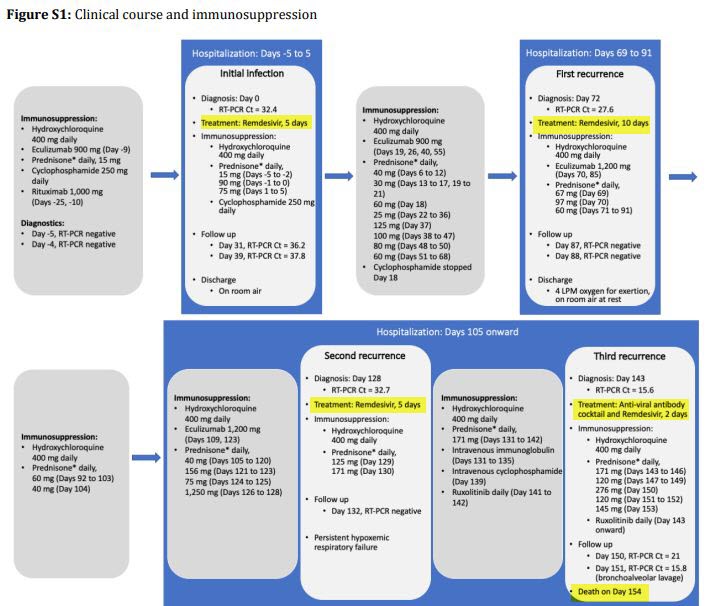
Dead on Day 154
- Day 0: Patient in 40’s was admitted with fever and nausea, reporting ‘chills, muscle aches and headache three days prior to hospitalization’ and subsequently developed ‘dizziness, nausea, abdominal pain, anorexia and persistent fevers’.
- Day 0: 2 x Negative PCR-Tests, then a positive RT_PCR with CT of 32.4!!
- Use of Hydroxychloroquine 400 mg daily – (without combining with Zinc & Azithromycin – what’s the logic here, just for reduced inflammation perhaps?) (29) (30) (31) (32) (33)
- Use of Prednisone – only 15mg – what’s the point?
- Day -5-5 – Remdesivir for 5 days
- Day 72 – Remdesivir for 10 days
- Day 128 – Remdesivir again for 5 days
- Day 143 – Remdesivir again for 2 days
- Day 150 – Patient intubated
- Day 154: Death

52 patients with PCR-confirmed COVID-19 diagnosis, who were hospitalized between March 15 and June 8, 2020. – This paper does not mention what treatment these patients received (even in the supplementary data), but 12 of these patients died, and all patients in study were selected because they were “covid-positive” patients with kidney involvement / kidney dysfunction, and at that time, Remdesivir & Ventilators were the go-to treatments. High SARS-CoV-2 Viral Load in Urine Sediment Correlates with Acute Kidney Injury and Poor COVID-19 Outcome (36)


Dr. Richard Bartlett interviews Jeremiah Skiba
Dec 2022 Rumble
The book about Rob Skiba who was murdered on October 13, 2021 by the deadly COVID Protocols. Rob and his family were completely aware of how deadly Remdesivir and the Ventilators were, and requested Budesonide (corticosteroid Pulmicort). The medical staff refused Budesonide, gave him Veletri and Remdesivir against his wishes, and put him on a ventilator, as well as administering 100% oxygen on a ventilator which the post-mortem said had shredded his lungs to the point they did not even look human. Even worse, these evil “trust-the-science-fiction” medical professionals kicked his wife and son out of the hospital and they had to try and advocate for him, by text messages, and without being able to see him.
Locking families out, allowed this nightmare to happen to God-knows how many people around the world. It’s why the doctors-nurses etc. stayed in Zombie-land. trying to put everyone immediately on a ventilator, administer the experimental emergency-use-authorized-only dangerous lethal drug Remdesivir, and ultimately raise the death numbers for whoever is doing this to our world, greedy psychopaths with their own agenda who have captured the medical industry, The medical staff become “group-think-protocol-followers”, and have to switch off their conscience to continue to do their job – in the hospital world, it looked like a pandemic because they “created” a pandemic because their protocols killed.
Family coming in do not get to “watch over or question the care” or advocate in person to ensure they are getting everything they need, or become an advocate bed-side to try and get through to the medical staff about these deadly treatments. Staff come into work, understaffed, under prepped, told they are facing a pandemic, and have their own fears about that, getting harassed and mind-controlled by administrators, and getting protocols “dictated” to them. They have no contact with any voice of reason, logic, or from the hearts of people that actually care about the patients. These brainwashed people faked consent on forms – which would never happen in a non-covid-psychosis world. #WeWontForget
From his wife’s site: https://theprotocolthatkills.com/ :
A True Story and Urgent Warning
I never thought I would be writing the tragic and true story of how my husband suffered and died at the hands of a group of “medical professionals”—a totally callous and insensitive group who indiscriminately follow what I learned is a government-incentivized “protocol that kills.”
I found the video above because I found a really amazing video created by Rob but spoken by his family, and when I went to the channel to see what other videos they had, I discovered he had many, many great truth-seeker videos, and I discovered from the comments that he had died from the COVID protocols. I then went to his websites and found his twitter account, which led me to discover both his wife and son had written books about their ordeal with the medical mafia to both honour Rob and warn the public. They are currently creating a documentary, a memoir, and a legal brief.
Jerimiah (Rob’s son) wrote his personal account, in a book called “Never got to say Goodbye“.
See also:
Posts tagged “Fauci” | Solutions-Health | Rigged-Science

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:
 Aussies
Aussies Or Buy me a Coffee (PayPal)

References

![[1979] Social Influence Mind Control (ONR)](https://pennybutler.com/wp-content/uploads/2022/12/OfficeNavalResearch-ResistSocialInfluenceHL-677x437.jpg)