[Must See!] Aussie GP – Dr Melissa McCann – Stands up [Part I]

THIS IS OUTRAGEOUS. This is a must-listen-to important speech by QLD GP Dr. Melissa McCann. UNBELIEVABLY TRAGIC & CRIMINAL. (Video + Transcript + Screenshots + REFS)
(Darn it, my host can’t handle the size of this post, split into two Parts. See also—Part II)
Dr. Melissa McCann Speech
Dr Melissa McCann, BPharm, MBBS, FRACGP, Graduate Certificate of Allergic Diseases – Whitsunday Family Practice | @drmelissamccann | Doctors Against Mandates, Australia | Telegram
Good evening Sydney. I’d just like to welcome you all here this evening. My name is James Lutton, and I’m a member of the United Australia Party team that have helped house these events for you. Craig Kelly will be your guest MC this evening.
Thank you so much, and what a wonderful crowd we have tonight. As you’re all aware, the COVID-19 pandemic response has divided opinion around Australia and the world, but as a former leader of the United Australia Party, Sir Robert Menzies once said, today’s truth is frequently tomorrow’s error. If truth is to be triumphant, the process of free debate must go on, and that is the spirit that we’re here in tonight. Now we know there have been many adverse effects attributed to the COVID-19 vaccines, which until recently have had limited publication. We’re here today to assist in the understanding of the COVID vaccines and the side effects of this so-called immunisation. To get the ball rolling, our first speaker tonight is Queensland GP, Dr Melissa McCann. Dr McCann comes from a pharmaceutical background, is a registered general practitioner and a practice owner. She is an incredible woman with an incredible story, and trust me. She has some extremely important information to share with us all tonight. Dr McCann started as a pharmacist working on before commencing postgraduate medical education in Western Australia. Since completing her medical training, she has worked around Australia and has now settled on the Whitsunday coast where she has built a reputation as a caring and highly competent general practitioner. Please give a big welcome to Dr Melissa McCann.
Thank you so much, everyone, and thank you, Craig, for such a generous introduction. I just want to start this final talk tonight by sincerely and humbly thanking Mr Clive Palmer and the United Australia Party, for so generously hosting this important event. It has been an absolutely humbling and so hopeful to have spent a few days with this incredible professional and competent group of people, the other international expert speakers, Dr Peter McCullough and his beautiful wife. Dr Pierre Kory, and Mr John Leake.
And also, Mr Clive Palmer’s amazing team. I actually don’t know how this incredible team has managed to pull off this event, but I do know that these people literally should be running this country. They are the most capable, dedicated, caring and professional team of people that I’ve ever worked with, and we’ve been so generously accommodated by Mr Palmer, and I’ve been struck by the thought that someone with the vast resources and influence that he has, he could much more easily be bunkering down on a luxurious private island with his family and friends, whilst the rest of us face whatever dystopian future the unelected elites have planned for us, and instead, this quite incredible man has cared enough about the fate of his fellow Australians to challenge the COVID narrative and to use his resources to support the vaccine injured and to provide this forum for all of us to share the truth.
So from the philosopher Arthur Schopenhauer:
All truth passes through three stages. First, it is ridiculed. Second, it is violently opposed. Third, it is accepted as being self-evident.
As I consider this truth self-evident, I will speak as such.
I will be discussing severe adverse events and deaths following vaccines, and I apologise for any distress that may cause. So 2020 to 21, to me, was defined largely by fear, media images of coffins, body bags, and ICU scenes out of Italy and Wuhan, and stories of healthcare workers dying from COVID.
Next, the somewhat threatening statement from AHPRA, the regulator for all health practitioners on the 9th of March 21, which brought a new type of fear that any discussion unfavourable to the COVID vaccine programme could be career-ending. (01) (02)


I think it’s true to say that despite all of that, we first look forward to the COVID vaccine and that for the most part, doctors, nurses, and healthcare workers were first in line for ourselves, our parents, and grandparents, myself included, but as the programme rolled out more broadly in my rural area from around the end of 21, I started to see more adverse events than ever before.
For context, my clinic has always given a lot of vaccines, and has deliberately encouraged childhood and flu vaccines for many years by offering these to all patients without any fee.
For the COVID vaccines, I incidentally did very few due to the arrangements for pharmacies, and the government funded respiratory clinics to do these, and from around the end of 21, none at all.
My patients would still come in after having had their vaccine given elsewhere, and I had never seen anything like this.
One young patient with extensive blood clot after vaccination, several patients with strokes, patient after patient with miscarriages, and these at later gestation requiring DNC.
Patients with chest pain and unusual debilitating neurological symptoms.
In one week, four patients with confirmed myocarditis. In a region with a population of maybe 15,000, and my patient group, just a small fraction of that, the numbers just did not add up. By chance, maybe I would see one.
Multiple cases of myocarditis? This was impossible.


So in mid-November of 21, I sat down to do an informal practice audit, and look at some of those adverse events, and found there was a clear increase compared to previous years.
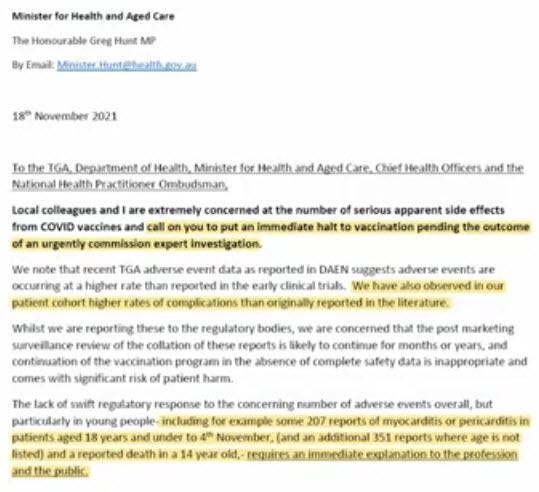
I went on to the TGA DAEN database and was horrified to see the reported death in a 14-year-old, reports of cardiac arrest in teenagers, at least some of those with death as a reported outcome.
Case after case of severe cardiac events in young people.


And literally thousands of severe events, strokes, blood plots, neurological events, blindness, heart attacks….
So I immediately wrote to Minister Greg Hunt and Prof John Skerritt describing what I had observed in my patients and highlighting this serious adverse event on the DAEN. I requested the immediate suspension of the vaccination program and a review of the safety issues. (03)
From John Skerritt the response:
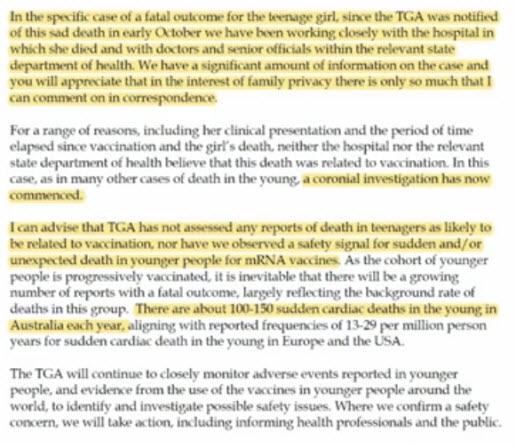
“For the fatal outcome of the teenage girl, they did not believe the death was related to vaccination, and there was no safety signal for sudden or unexpected death in young people.” He advised that there are around “150 sudden cardiac deaths in young people each year, so it was inevitable that there would be growing numbers of reports of death to the database,” and finally, “the TGA’s focus remains on keeping Australians as safe as possible from a dangerous and very contagious virus that has killed millions of people globally.”

Frankly, I would have preferred the TGA’s focus remain on the vigilant and competent regulation of therapeutic goods, including adverse events surveillance, and I think I was naïve enough then, that I was quite put out by this response.
To compare, in 2010 in Western Australia, the halting of the childhood flu vaccines after several nurses and doctors had noticed an increase in events such as Febrile convulsions compared to previous years, a detailed report later reviewed the timeline and within weeks the program was suspended. (04) (05)
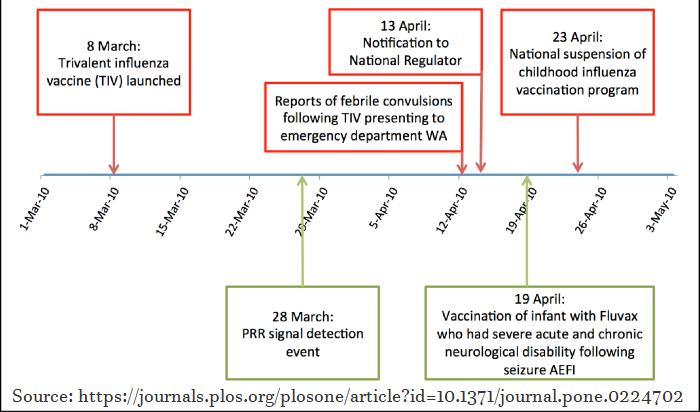
The safety signal was identified based on the reports of just a few doctors and nurses recognising a change to the usual pattern of events and an increase in the proportionality reporting ratio.
This ratio is one way of comparing reports to the database from a particular product compared to similar products and takes into account the number of doses given.
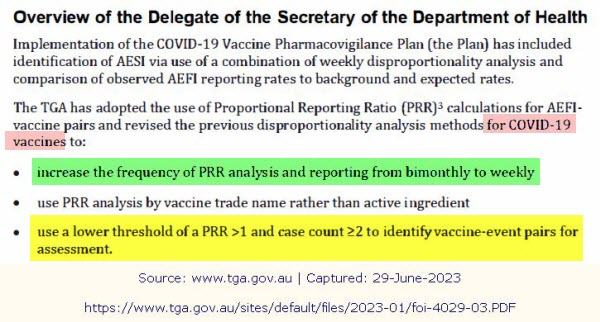
Normally, a ratio of more than one suggests a higher than expected rate of adverse events. In fact, prior to the COVID vaccine rollout in Australia, a ratio of one was selected to allow for faster detection of signals and the ratios were to be reported weekly rather than bi-monthly.
| 9 January 2023 | COVID Pharmacovigilance activities including ACV and VSIG minutes. (06) |
| FOI 4029 | FOI 4029 document 1 (pdf,184kb) FOI 4029 document 2 (pdf,173kb) FOI 4029 document 3 (pdf,228kb) FOI 4029 document 4 (pdf,186kb) FOI 4029 document 5 (pdf,152kb) FOI 4029 document 6 (pdf,278kb) FOI 4029 document 7 (pdf,81kb) FOI 4029 document 8 (pdf,122kb) FOI 4029 document 9 (pdf,250kb) |
| FOI 4029 document 3 (pdf,228kb) (see p.10) | Advisory Committee on Vaccines Minutes Meeting 25, held 29 September 2021 COMMITTEE IN CONFIDENCE TRIM Reference no. D21-3141615 (07) |
Documents recently released on the freedom of information show this analysis was not done weekly but continued by monthly and show ratios of not only more than one but well over two for cardiac arrest for the vaccines across the period.

| 29 November 2022 | Proportionality Reporting Ratio analyses for the COVID-19 vaccines to 22 October 2022 (08) |
| FOI 4032 | FOI 4032 document 1 (pdf,88kb) FOI 4032 document 2 (pdf,324kb) FOI 4032 document 3 (pdf,241kb) FOI 4032 document 4 (pdf,165kb) FOI 4032 document 5 (pdf,217kb) FOI 4032 document 6 (pdf,315kb) FOI 4032 document 7 (pdf,285kb) FOI 4032 document 8 (pdf,220kb) FOI 4032 document 9 (pdf,197kb) |
For other serious events such as intestinal ischemia, pulmonary infarction, ratios of more than 20 and up to 50 during the time of highest uptake, ratios over 20 for myocarditis again during the peak of the vaccine rollout, rare and serious events such as vertebral artery dissection, aortic dissection and rupture, aneurysms, strokes, intracranial haemorrhages were shockingly high given these are such rare events. (09)
Compare again with just 11 years prior, with the reporting ratio just edging over two, and within one month of that signal being detected the national suspension of the program.
In addition, deciding causality versus coincidence does not just involve looking at ratios or background rates. The WHO Handbook for Adverse Events Surveillance, provides a simple method and a flow chart.

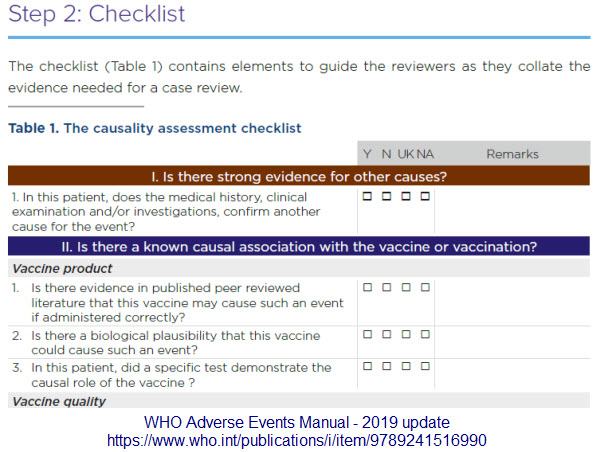
- WHO User Manual Adverse Events 2019-2021 Edition (see p.22) (10)
- WHO User Manual Adverse Events 2018 Edition | PDF (see p.26) (11) (12)
- WHO User Manual Adverse Events 2013 Edition (13)
For example:
- Is there a strong temporal relationship? That is that the event started soon after the vaccine.
- In this patient can we confirm another cause for the event?
- Is there evidence in the published literature that the vaccine may cause such an event?
- Is there a biological causeability that the vaccine may cause such an event?
Complicating the issues was that even doctors who had themselves had severe adverse events often remained of the belief that they should not discuss their often life-changing events with others, and that they should continue to encourage vaccination, and so these doctors and other health professionals suffered in silence, unable to even discuss with their own colleagues for fear of ridicule or reprimand.
It has been near impossible to have any honest, open discussion about the harms the vaccines may cause due to AHPRA statement, media censorship, and conflicting advice from official sources.
Mandates in this or any environment were and are a catastrophe of medical ethics that deserves a talk all of its own.
I saw patients who had presented months after the vaccine with ongoing chest pain and breathlessness, especially when they exercised, who resorted to paying a $1,000 to have an MRI done privately, and finally, they would get a diagnosis of myocarditis—months and months after vaccination—and I often reflected that had these patients died from a heart attack or a cardiac arrest at any point in the months between the vaccine and finally getting an MRI and the myocarditis diagnosis, that there is no way that their death would have ever been attributed to the vaccine.
With the astonishing excess death rates in Australia and around the world, I wondered just how many people this or something similar might be happening to. (14) (15) (16)

I would describe waking up for me, the way John Green described falling asleep or falling in love — “slowly, and then all at once,” and in 2022, I woke up and all at once.
In March of 2022, I wrote to Minister Hunt and John Skerritt again, this time with 14 other doctors from various specialties co-signing again requesting in the strongest terms the immediate suspension of the program and a review of the safety issues. (17)

In summary: I wrote to Minister Hunt and John Skerritt in November 2021 requesting immediate suspension of the covid 19 vaccination program and urgent review of the safety issues. I presented a number of reports from the DAEN database, and also described a number of safety issues that had been observed in m y rural patient cohort which were vastly in excess of expected rates based on the published literature and the TGA weekly safety reports. I do not consider these concerns were adequately addressed, and in the three months following this correspondence colleagues and I continue to observe high numbers of adverse events amongst our patients and we remain extremely concerned regarding the adverse events reported on DAEN, including many with death as a reported outcome.
I request in the strongest possible terms an an immediate suspension of the covid 19 vaccination program pending an urgent review of the adverse event reports. The high number of observed adverse events constitute a serious safety signal and in my view, continuation of approval represents an abrogation of our duty of care in relation to medication safety and regulatory approval.
Dr Melissa McCann, 20 Mar 2022
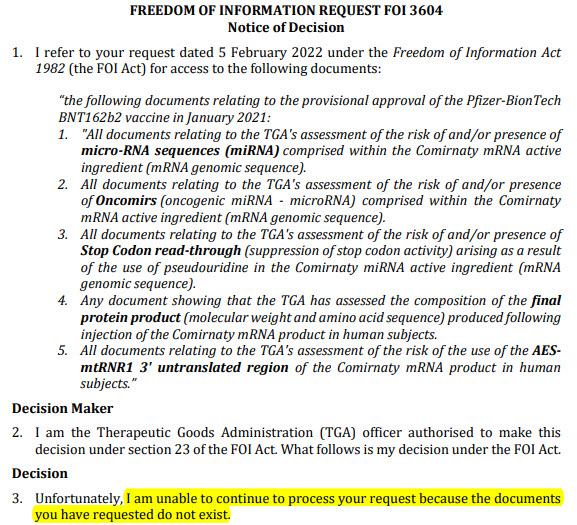
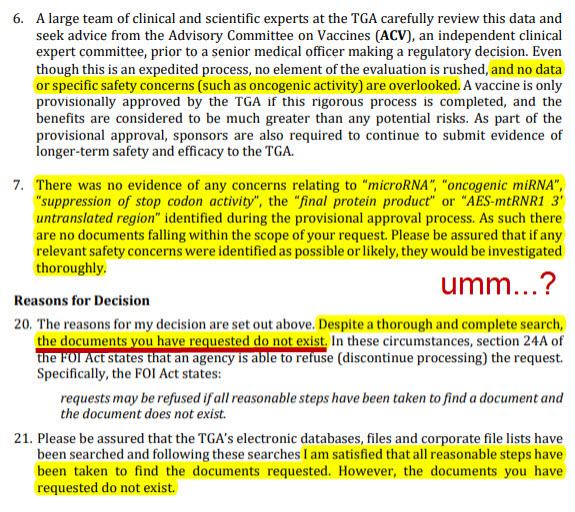
I raised again the reports of cardiac events and the risks potentially related to the genetic sequences of the vaccines, including risk due to impacts of microRNA sequences and potential Oncomir’s, which are small RNA sequences that cause cancer, and for which the TGA acknowledged in a freedom of information response that they had not evaluated. (18) (19)
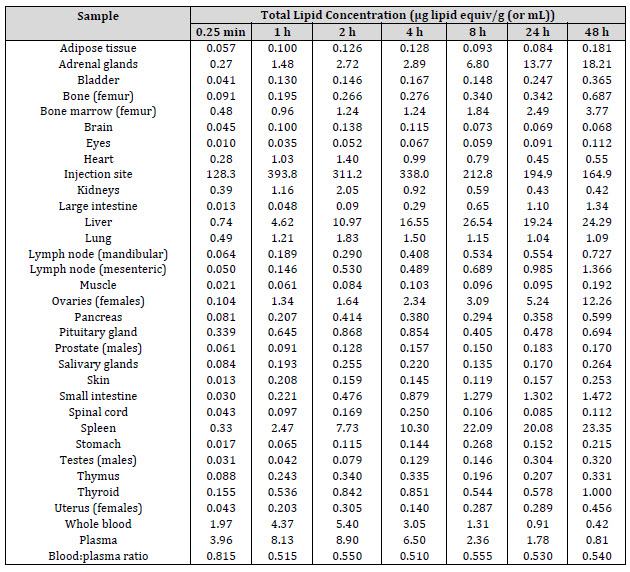
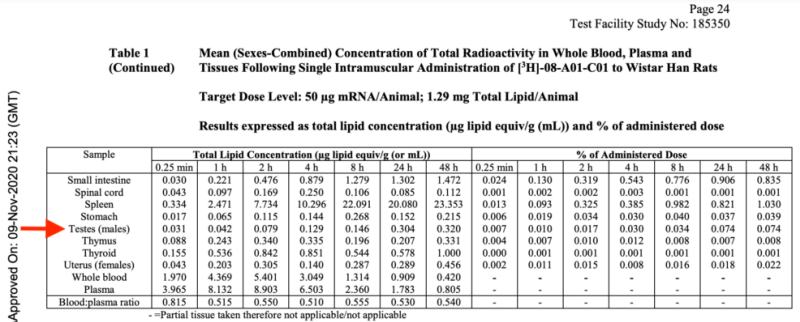
I raised the unknown metabolism of the lipid nanoparticle adjuvants, and these metabolic animal studies were stopped at just four hours in animals, and at that time, almost none of the lipids had been metabolised from the liver at all—how long these products stay in the body or their metabolic pathway is entirely unknown! (20) (21) (22) (23)
These are highly inflammatory and cross the blood brain barrier and into the neuro tissues, into the spinal cord, into the ovaries and the testes, and of course, genotoxicity and carcinogenic studies had not been performed with dubious justification for this oversight, in my opinion, which also deserves another talk all to itself. (24) (25)
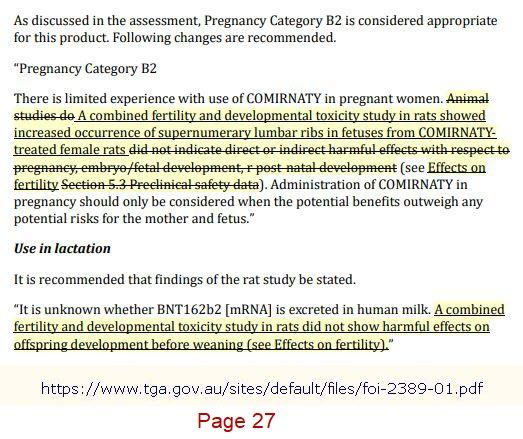
Finally, I raised the concerns of safety and pregnancy, and with an assessment obtained by freedom of information, (26) first suggesting a Category B2 for the Pfizer product, noting the abnormalities in the animal reproductive study of supernumerary, lumbar ribs in foetuses from COMIRNATY-treated female rats, which then, without explanation, was revised to remove this sentence and to change to a category B1 in the publicly available product information, (27) (28) and the preclinical studies also demonstrate a number of other foetal anomalies and a doubling of the risk of miscarriages in these animal studies, and this reflected what I was seeing in my patients.(29) (30) (31) (32) (33)

[Must See!] Aussie GP – Dr Melissa McCann – Stands up [Part I]

More Videos on TGA FOI 2389 [Dr. John Campbell]

TGA FOI 2389 – BigPharma & TGA Conflict$
TGA FOI 2389 – Ingredients, Dosage, Manufacturing
TGA FOI 2389 – No Benefit
TGA FOI 2389 – Safety Studies Skipped
TGA FOI 2389 – Spike protein in any cell in the body
TGA FOI 2389 [Video & Doc]
Unsatisfied with the responses of coincident adverse events and deaths following vaccination, I undertook a freedom of information requests process with the TGA, and following an unexpectedly arduous consultation process, I received 10 documents containing the TGA causality assessments. Amongst them:
- a 21-year-old female who died from myocarditis and cardiac arrest with the assessment outcome awaiting, which has since been determined, causal by VC, and now appears on the TGA safety report
- this beautiful young lady named Natalie died after a long and traumatic ICU battle with weeks on ECMO after developing vaccine-induced myocarditis. She was in her final year of law school and just two weeks after her 21st birthday when she died. Today would have been Natalie’s 23rd birthday, and instead her mother and brother are spending her birthday today grieving her life lost too soon. (34)


- I also received the case report of a 14-year-old female who died and the assessment decision—unlikely causality
- A 21-year-old male who died and the assessment outcome decision was—question mark ? causality
- A 24-year-old female who died of cardiac arrest where the assessment decision was—causality
- A 9-year-old child who died of cardiac arrest and the assessment outcome decision was— causality
- A 7-year-old boy who died of cardiac arrest and the causality outcome decision was—causality
And just to be completely clear, I requested these documents under freedom of information because I wanted clarity on the TGA assessment of the reports of deaths. I was confused that the safety report say 900 plus cases of death but only 14 confirmed causal. (35) (36)
| 22 July 2022 FOI 3727 | TGA Case Assessment summaries in relation to specific case numbers on the Database of Adverse Event Notifications (DAEN), and data on the numbers of adverse events reported to Pfizer. FOI 3727 document 1 (pdf,155kb) FOI 3727 document 2 (pdf,181kb) FOI 3727 document 3 (pdf,97kb) FOI 3727 document 4 (pdf,92kb) FOI 3727 document 5 (pdf,130kb) FOI 3727 document 6 (pdf,129kb) FOI 3727 document 7 (pdf,317kb) FOI 3727 document 8 (pdf,97kb) FOI 3727 document 9 (pdf,136kb) FOI 3727 document 10 (pdf,133kb) FOI 3727 document 11 (pdf,890kb) |
When I discussed this with other medical colleagues, they all draw the conclusion that all the other deaths have been reviewed and are not causal. But the language is misleading. The TGA implies this but does not explicitly state this. So I was requesting the actual TGA assessments of these reports of death, and these documents are factal adverse events, team meetings. The names are redacted but there are multiple people present at these meetings, and the opinion of this TGA team in some of these cases, including in young children, was causal. (37)
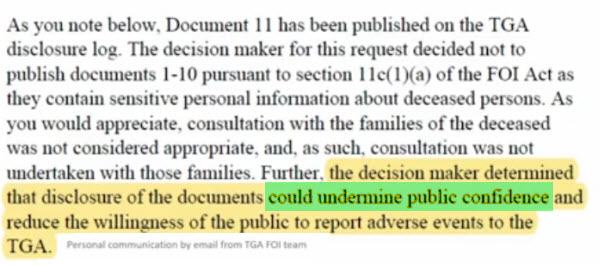
Or in other words, the vaccine is the likely cause of death, and when I asked the TGA freedom of information team why these documents were not published to the public disclosure log, I was advised the decision maker determined that disclosure of the documents could undermine public confidence, and reduce the willingness of the public to report adverse events to the TGA.
This is outrageous.

Doctors and the public have relied on the fact that out of millions of vaccines—only 14 deaths—and this appears to be completely misleading and deliberately non-transparent to the public.
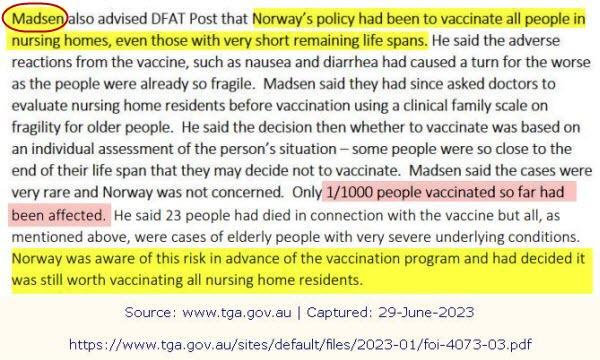
Before the vaccine roll out, there were also reported deaths in the elderly in Norway, and the media release by the TGA in January of 21 announced that an investigation into these deaths was underway. (38) (39)
Three weeks later, the investigation was complete, and there was no causal link between vaccination and the deaths in the elderly. (40)
I recently obtained under freedom of information the correspondences related to that investigation:
These report the Norway regulator stating that adverse reactions from the vaccine, such as nausea and diarrhoea, had caused a turn for the worse as the people were already so fragile and that one in 1,000 people had died, (41) (42) and John Skerritt wrote that for the 30 fatal cases, a uniform picture, nausea, vomiting, diarrhoea leading to acute kidney injury in frail patients. (43) (44)
See: Part II

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:
 Aussies
Aussies Or Buy me a Coffee (PayPal)

References
![[RANT] Explain why they’re counting the “Jabbed” as “Unvaccinated” [ChatGPT]](https://pennybutler.com/wp-content/uploads/2022/01/3-dose-anti-vaxxer.jpg)

![[RANT] I’m really nervous about what the tv is doing to my friends](https://pennybutler.com/wp-content/uploads/2021/09/mass-psychosis-cause.png)