RW 2/8). US Healthcare Framework & EUAs

This section is on the US Healthcare Framework & Emergency Use Authorization (EUAs)
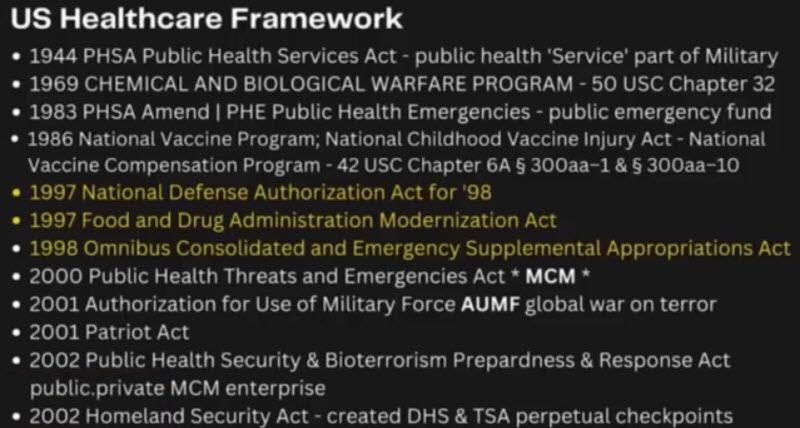
- 1944 Public Health Service Act
- 1969 Chemical and Biological Warfare Program
- 1983, Public Health Services Act amendment
- 1986 National Vaccine Program, National Childhood Vaccine Injury Act, National Vaccine Compensation Program
- 1997 National Defense Authorization Act
- 1997 Food and Drug Administration’s Modernization Act
- 1998 Omnibus Consolidated and Emergency Supplement Appropriations Act
- 2000 Public Health Threats and Emergencies Act.
- 2001 Authorization for use of military force under Bush, and this was the AUMF (Authorization for Use of Military Force)
- 2002 Public Health Security and Bioterrorism Preparedness and Response Act,
- 2002 Homeland Security Act
I’ve split up Rebecca Walser‘s “Unravelling the Web of Globalization & the Totalitarian Control of Humanity” video into bite-sized sections, because she explains it so well, and I truly want to help people come across this information and understand it, so I’ve broken down her “Militarization of Global Health” section of her video into 8 parts, which I’ve transcribed and made into separate posts.
Militarization of Global Health: US Healthcare Framework
23 Feb 2023 Rumble | Telegram (19mins)
Full Video: Rumble | YouTube | WalserWealth
Transcript:
So, what we’re talking about is the public monetization and militarization of healthcare that has really occurred post-9/11, and to continue our Etch-a-Sketch framework, we’re going to break this down into two areas: domestic United States laws specifically, and then we’re going to look at the global framework that is also guiding the U.S laws and, really, I would say at this point, beginning to control U.S law.
So, we’ll start with domestic.
The first thing I want to talk about is the timeframe here, and this is going to take a little bit of time, but this is really the piece that we are not understanding, and that I’m highlighting, and I will just want to say that Katherine Watt, who really is a legal researcher, an author, she has a substack called Bailiwick News, she has been a phenomenal academic resource in this arena, and I’m certainly not in any way trying to emulate her work. I’m trying to bring it into more of a direct light, directly connecting these dots for you guys and actually showing you the actual laws, which I think is quite alarming.
The first thing I want to go through is this 1944 Public Health Services Act, which really set up public health as a service as part of the military, and so, that was really early on, and I mean it’s the same year as Bretton Woods, but basically, this was the beginning framework of public health and it being an actual entity and group. (01)
And then in 1969, we had the Chemical and Biological Warfare Program, and we will look at that, but that is 50 USC Chapter 32, and specifically, the Chemical and Biological Warfare Program really began sort of what people are calling a false justification or a false dichotomy that we needed to set up or have programs related to CBRN, which stands for Chemical Biological Radiological and Nuclear elements, and classifying and labelling those developments of those elements was defensive. It was for defensive purposes. It was prophylactic or it was protective. (02)
So, we started this framework in 1969 in healthcare that basically said we need to implement this CBRN program because we need to protect ourselves in case anybody else does, and that is, on its face, ridiculous. You’re going to develop advanced chemical, biological, radiological or nuclear weapons because somebody else is also going to do it, but all of these types of things are active, they’re aggressive. They’re not retaliatory, they’re not defensive. They’re actually aggressive, they’re in the affirmative. So, that just set up a framework that’s a little bit false.
In 1983, we had a Public Health Services Act amendment that really created for the first time PHEs, or public health emergencies. It also created a public health emergency fund that was publicly funded, that could be, at the time, was only $30 million. Basically it was the ability of the government to have a fund that could be disseminated quickly to deal and target public health emergencies. Nothing unusual or nefarious. Like I said, all these things can be rationalized individually, and it’s only when you put the Etch-a-Sketch framework together that you can see, “Whoa, wait a minute, what has happened here?” (03)
In 1986, this was probably one of the most seminal pieces of healthcare legislation that has really happened in the United States, and that was the introduction of the National Vaccine Program. Basically, saying we want these kids to have these vaccines on these time frames, that was really the beginning of that. It also was the beginning of the National Childhood Vaccine Injury Act, which created the National Vaccine Injury Compensation Program. (04) (05) (06) (07)
So basically, people don’t understand, even to this day, even as much work as Robert Kennedy has done on this with his Children’s Defense Alliance, that basically, vaccine manufacturers were avoiding liability from developing these types of protocols that were requested by Health Services. It was not going to happen because manufacturers were too afraid of whatever potential liability could come, and so they weren’t going to do that. Obviously, you can’t have a healthcare system where no private entity will create any kind of therapeutics because they’re afraid of liability if it’s a new therapeutic. So, we got this concept of, “Well, we have to shield them from liability because otherwise, they won’t create it. It won’t be commercially viable,” and that framework is very important for what has since happened post-2020. So, we’ll come back to that, but it was a really big framework, and it is something that, you know, there’s so much literature on it, and still, people just don’t understand it.
Then, I have these three acts together: the 1997 National Defense Authorization Act, the 1997 Food and Drug Administration’s Modernization Act, and the 1998 Omnibus Consolidated and Emergency Supplement Appropriations Act. All of these things really started to expand access, and again, you could just do podcasts on just these acts, but I just want to give you the highest level possible where you can see the framework and finally understand what is going on here.
In 1997-98, there were some court cases that were going on between untested Anthrax interventions that were being used to help protect the military and deployments where they thought that this would be a biological agent that would be used. There were some cases that were brought to the courts about using these unapproved products directly on the military. They expanded the ability to be used on the human population overall. I know that’s unbelievable, but I will show you the actual laws directly so you will be able to see exactly what happened.
The other thing they did is they took the stockpile of weapons and the CBRN category (chemical, biological, radiological, and nuclear) and relocated them from the Defense Department to Health and Human Services and renamed them “pharmaceutical stockpiles for emergencies.”
It all makes sense, but when you start to put the pieces together, you say, “Wait a minute, we’ve just moved sort of weaponized military use and items into healthcare.” The Health and Human Services, which really just controls healthcare for the United States citizenry, has nothing to do with militarization, so it’s a little alarming.
Then you have the 2000 Public Health Threats and Emergencies Act. This really set up what the beginning of MCM (Medical Counter Measures), and this becomes really huge. This Medical Counter Measures is a legally defined term of automatically Medical Counter Measures, and when you’re dealing with Medical Counter Measures, you have new frames of legal protections or lack of legal protections because these are countermeasures, so we will go through that. (08)
In 2001, you have the Authorization for Use of Military Force under Bush, and this was the AUMF (Authorization for Use of Military Force), and this really was the beginning of what we know to be the “Global War on Terror”. This sort of set the world potentially as a potential enemy combatant, and that you would have different enemy combatants. There’s an actual famous United States Supreme Court case that we’ll discuss when we go through that. (09)
In 2002, you have the Public Health Security and Bioterrorism Preparedness and Response Act, and this really set up sort of like a Fannie Mae and a Freddie Mac a Consortium of a public-private enterprise that dealt with medical countermeasures to deal with public health and safety.
You have the 2002 Homeland Security Act, which created the Department of Homeland Security and then the Transportation Safety Administration as a division of the DHS. That sort of set up like these perpetual TSA checkpoints and kind of put us in almost a perpetual state of militarization, if you will, of living in America.
So let’s go through some of these things that I really want to pull out for you. This is USC 50 USC chapter 32. (10)
This is the 1969 Chemical and Biological Warfare Program, and I want to pull out here for you 1520a, which is the restrictions on the use of human subjects for testing of chemical and biological agents. (11)
Remember when I said in 1997, and 98, there were some court cases, and they really, through those three laws, pulled back the ability to use untested medical interventions and protocols on the military. They expanded that to all humanity, so all Americans, all humans, period, and so here are the restrictions of using human subjects for testing on chemical and biological agents. I want you to see that this says:
“The Secretary of Defense may conduct directly or by contact any test or experiment involving the use of a chemical or biological agent on a civilian population or any other testing of a chemical agent, biological agent, on human subjects except in Part B, which is exceptions, subject to C, D and E, the prohibition set in subsection a.
Which means that:
“the Secretary of Defense may not conduct these experiments of chemical or biological agents on civilian populations or human subjects. They may not conduct that, unless that test is being carried out for the following purposes:
- Any peaceful purpose that is related to a medical, therapeutic, pharmaceutical, agricultural, industrial, or research activity.
- Any purpose that is directly related to the protection against toxic chemicals, biological weapons, and agents.
- Any law enforcement purposes, including any purposes related to riot control.
What they’re saying is you actually can test chemical and biological weapons or agents on a civilian population if you’re doing it for a peaceful purpose that is related to a medical activity.
So post-2020 coronavirus, we absolutely have that situation where we have a new global pandemic for the first time, and we are going to have the federal government under the Secretary of Defense, the Department of Defense able to actually test chemical and biological agents on a human civilian population because it is for the peaceful medical purpose related to disseminating. You could also look at even number two that is directly to protection against toxic chemicals and herbological weapons or agents. You know we don’t even truly know what this actually is or was to this day that will be coming out. Ouch when I tell you that will be coming out, it will be coming out. So you will see that even two could actually apply. And then you know three is not really applicable.
So when you start to see the actual law and writing on paper, you start to realize, “Wow, wow, and wow.”
Emergency Use Authorization (EUAs)
So here is the introduction of the EUA, the Emergency Use Authorization, and this was, in fact, the actual impetus for me as a lawyer.
This was the actual impetus for me as a lawyer to go down this rabbit hole because I understood that an EUA authorization had two specific parameters that needed to be met in order to be legally affected.
The first thing was that there could be no alternative. So if you approve a medical protocol through any EUA authorization, that can only legally happen if there’s no other medical protocol intervention. So when we early on saw that a lot of doctors were coming out and talking about alternative early intervention treatment and therapies for specifically coronavirus…and you guys remember, The Lancet had a report about the ineffectiveness of hydroxychloroquine, ivermectin, since retracted. (12)
But many doctors came out and said, “Hey, listen, between, you know, early intervention with some kind of bronchial steroids, hydroxychloroquine, or Ivermectin, which interferes with the ability of the virus to actually attach to the receptors.
They had to not have those therapeutics take be considered a viable medical protocol intervention for coronavirus. Otherwise, if that had not happened, you would never have an EUA authorization approved because there would be alternatives, and you would not need to go to the extreme of an emergency use.
So that tells you something right there, that tells you that an Emergency Use Authorization is a very, very, very low bar, and it makes sense. Again, all of these things make logical sense.
You need to have the ability, in a legal framework, to introduce a potential fix, cure, a medical cure that you know in an emergency situation that won’t allow for the standard six to ten years of protocol testing, development, retesting, re—you just don’t have that framework of time. So you have to fast track everything and because you have to fast track everything. Of course, you’re not going to go through traditional medical testing and protocols that are longitudinal and years in nature, and so EUA makes sense, but specifically with coronavirus which you saw, and this has since been completely validated in writing and substantiated, and I could never add all that into this presentation, but you can go out and look at the Twitter files and specifically look at, and even Congressional hearings since the beginning of this year have shown that they absolutely censored some of the largest, most well-reputable doctors from Harvard, Stanford, and Yale talking about alternative in the early therapeutical interventions and and and saying, “No, no, no, no, no, no.” (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32)
And that really set up the ability for whatever therapeutic they were going to come up with eventually to get an Emergency Use Authorization.
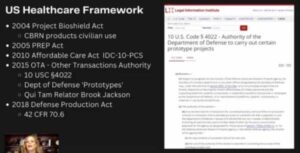
That being said, I have these up here because I want you guys to actually see what they are. This is 21 US Code Section 360bbb-3 – Authorization for medical products for use in emergencies. (33)
Basically, what you can see is that notwithstanding provisions in this chapter and section 351 of the Public Health Services Act, which we already talked about, the Secretary may authorize the introduction of a drug, device, or biological product into interstate commerce during the effective period of a declaration under subsection B, intended for use in an actual or potential emergency as an emergency use authorization.
Under this paragraph, one may authorize an emergency use product that (a) is not approved, licensed, or cleared for commercial distribution under traditional protocols of health services.
So, what this is saying is that when we have an EUA, we do not have time for those traditional protocols, and we can bypass those and go straight for the ability to have this emergency intervention. Again, it makes complete sense.
Going back now through the list, I want to specifically talk about the Authorization for Use of Military Force that came about in 2001. (34)
This is a Brown University Watson Institute for International and Public Affairs analysis that was done in December of 2021. (35) (36)
You can see that it’s showing you all of the military interventions that have been authorized through this AUMF. The Global War on Terror Authorization of Military Force also ended up in a famous Supreme Court case from 2004, Hamdi v. Rumsfeld. (37)
Donald Rumsfeld was the Secretary of Defense at the time, and basically, Hamdi was a US citizen who had been detained as an ‘unlawful enemy combatant’ and challenged the legality of his detention. The Supreme Court actually rejected his argument that the President lacked authority to detain citizens and enemy combatants, holding that Congress’s enactment of the 2001 Authorization for Military Force authorized the President to do so. The court, though, did agree with Hamdi that due process entitled a US citizen who is detained in the United States as an enemy combatant to a meaningful opportunity to challenge his classification as a new combatant before a neutral decision maker. (38)
In other words, he had a procedural due process right to challenge his classification as an enemy combatant, but otherwise, if he is an enemy combatant, he was legally detained.
This is where you can start to see kind of what happened around 9/11 and the implications that came.
Emergency Use Authorization Cont’d
I just want to digress for a moment because I realized I didn’t exactly explain something. So, when the EUA, this was the nexus of how all of this, me going down this rabbit hole for the last really 18 months hard, but I would say really since March of 2020 came about, because I started having a problem once the therapeutics were being developed for EUA authorization related to the 2020 pandemic.
We started getting the word “mandates” associated with these therapeutics, and the problem that I saw immediately as a lawyer is that mandates were not possible because when you have an EUA authorization, because the testing protocols have been bypassed, it requires legally that the human subject, the person that’s receiving that medical intervention, give informed consent.
The legal definition of informed consent is that a person has been fully explained the risks of the therapeutic, and they waive, acknowledge, and then waive all of their legal rights regarding any repercussions, up to and including death.
So, if you actually read the informed consent waiver that you would have to sign for an EUA product, you will see that you actually are – it states right there that the protocols have been bypassed, and that you acknowledge that there are risks that are unknown at this time. It’s almost like an experiment, and it says that you are waiving your rights for any kind of compensation related to damages, up to and including death.
As a lawyer, I started grappling with the fact in 2021 that we were looking at EUAs being paired with mandates, which is legally not obtainable. You cannot force someone to take an EUA that requires them to waive all of their rights, even over their death. That is not legally reconcilable.
So, something else was going on. There was something else that was allowing that legal construct to happen. And that is the impetus for me going down, for the last, since March of 2020, into what is going on because healthcare obviously is not my area at all.
Full Series Militarization of Global Health:

RW 1/8.) Totalitarian Control of Humanity : Financial
RW 2/8). US Healthcare Framework & EUAs

RW 3/8.) Project Bioshield & PREP Act
RW 4/8.) OTA & Brook Jackson’s Pfizer Case

RW 5/8.) Forced Asymptomatic Quarantine
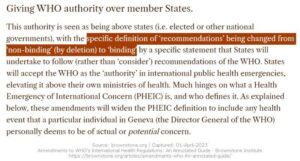
RW 6/8.) Global Health: WHO IHR Amendments

RW 7/8.) EUA Removal of Informed Consent

RW 8/8.) Final Words / Summary: Global Health Militarization

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:
 Aussies
Aussies Or Buy me a Coffee (PayPal)

References


![Advanced PCR Questions to ChatGPT [3/3]](https://pennybutler.com/wp-content/uploads/2023/02/PCR-777x437.jpg)