NZ C19-Vax Carnage Data Analysis [Dr Paul Oosterhuis]
- Updated:1 year ago
- Reading Time:47Minutes
- Post Words:12580Words

Australian Dr. Paul Oosterhaus visited New Zealand to look first-hand at the data from the NZ Whistleblower. This is their video together with Liz Gunn, analyzing the data before the whistleblower’s arrest.
M.O.A.R Data Analysis with Dr Paul Oosterhuis
30 Nov 2023 Rumble-Source (1.5h)
Welcome to you both. Dr. Paul Oosterhaus, I was on an Australian podcast with you, Cafe Locked Out. That’s where I met you first and you were very passionate about learning about the whistleblower’s data.
Well, I’ve been an opponent, well, I’ve been a proponent of that safety and somehow that makes you an “anti-vaxxer”, and the government hasn’t been forthcoming with the data. There’s been a lot of obfuscation and I’ve been waiting to get solid data that we can see the true effects and the true safety of the so-called vaccine or non-vaccine.
So before we get into that, can you give us a brief overview of your journey through the COVID-19 response? You, like many of us, have suffered greatly during this, haven’t you, for speaking out?
Yes. Well, I was an anaesthetist for 32 years. I worked in anaesthetics and critical care and so I had an interest in keeping people out of hospital, and early on I understood that COVID could be treated and I was passionate about getting the word out about early treatment, but I was also very critical about government policy on lockdowns and masks and I, in particular, was very concerned that children who didn’t have were being put at risk unnecessarily.
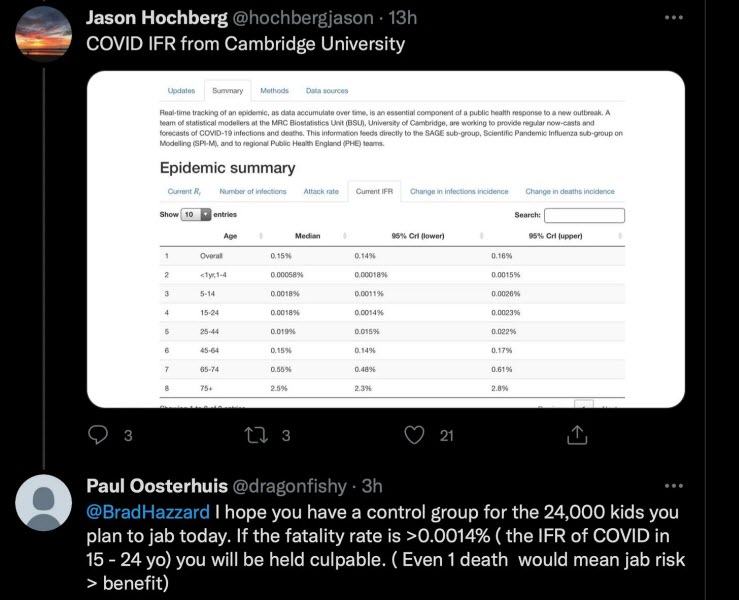
I tweeted the then health minister, Brad Hazzard, here in New South Wales, with the infection fatality rate by age and showed that these children, 24,000 high school kids who were being vaccinated on that day were not at risk of COVID, and said if there was even one kid that died from this 24,000, that you, Brad Hazzard would be culpable. (01) The Medical Board of NSW didn’t mention my Tweet’s to the Minister of Health https://pauloosterhuis.substack.com/p/the-medical-board-of-nsw-didnt-mention
Within two hours, I had become I was subject to a suspension hearing. As I went to the hearing, I gave my evidence, they ignored it and said, well, you’re guilty of violating the gag order, and I thought that was totally unacceptable because you cannot have informed consent with free discussion. People need to know both the risks and the benefits.
I warned the medical council that that they were breaching medical ethics, they were breaching the law, and so I subsequently sued the medical council and the Supreme Court of New South Wales, and they got my suspension, but I’ve continued to be a great critic of our government policy and of these synthetic gene injections, which they’re calling vaccines.
Winston Smith, I’ll call you, ironically, of course, if anybody knows Orwell’s book, 1984, Winston Smith, I came to you and I said, I believe that we should have a Trans-Tasman connection with this important data that you are bringing, not only to New Zealanders, but to the world, and I believe Dr Paul is a man to bring over, to have a look at the data. What was your first impression of him when we brought him over to New Zealand?
I just fell in love with a guy right from the get-go. He’s a beautiful human being, and yeah, he speaks from the heart and he’s got a lovely heart, and yeah, I really respect him for what he’s done. I respect the stand that he took, the courage and what he had to go through, and the tenacity to get it to get where he is now. It’s an honour to meet you, sir.
It’s more than mutual. It’s a great honour to meet you.
Dr Paul, when you came to New Zealand and you saw the data for the first time, take us into that. What was your reaction?
Well, I was holding back the tears, I think, was the first reaction because this is not just numbers. This is names, places, dates, and it’s not anonymous. It’s not anonymous. We’ve had data which has been obfuscated and made murky and that there are real names to each one of these, and the scale, the scale of the deaths both by site, by vaccinator. In our interview, you mentioned that there was a vaccinator that had 400 deaths, and I was blown away because that was way worse than Harold Shipman, who was the famous doctor (GP serial killer). So we have an autogenocide / democide, a crisis.
And they’re all unaware of it as well. They have no clue what they’re doing. I feel sorry for them. I honestly do. It’s genuinely not their fault. They believe that they’re doing the right thing, but it’s just got to stop, and it’s not the vaccinator’s fault per se. It’s who’s telling them, and it’s also, there’s a lot of things you can get into. It could be that the batch ID, where the site is located, the vaccination centre itself, and a million other factors that might point to why those numbers are so high at certain places, but yeah, the data is real. It’s 100%. It’s from the government. It’s the people’s data, and I strongly believe it belongs to them. I’ll protect as many names as possible. There will be no identifiable information on there, but the dates and times and locations, I’ll let the world see.
And that is a very important point to bring out at this stage. You had two rights, if you like, to weigh up. The right of privacy, the right of privacy of information, is one, that we accord great respect to in every society, but I believe, and I know that you agree with me, Winston, there is a far more important right that we must honour, and that is the right to expose criminal action by anybody, including by our ministers of the Crown, who are meant to be serving the people, and that is your courage to come forward and expose that. That’s extraordinary, Dr. Paul, isn’t it? It is an extraordinary level of courage that he’s showing.
Without this level of transparency, it would not be clear the scale of what is going on, and it was hard to believe until I actually met Winston and understood his involvement in setting up integral understanding where this data came from and setting up the database, and there’s just no question about the numbers that we have a lot of dangerous, deadly batches that would not be possible if this product was safe and effective.
Dr. Paul, can you go deeper into that? Because it is beyond any doubt that this no longer can be said to be of natural causes, or by chance, or this would have happened anyway, all these reasons that have been put about when people have died suddenly as a result of this jab. What does this data show beyond any reasonable doubt to you?
It shows that there are deadly batches. Numbers that just can’t be ignored, which makes it a dangerous product. There are lots of things that have come out already from the data and will continue to come out, but it didn’t protect Grandma—we know that there are a lot of elderly people died, and the thing without this record-level data, we wouldn’t have understood the time dependency, because we know exactly when the person was vaccinated and when they died, and the proportions, in some of these sites, it was worse than playing Russian roulette. These are incredible diff ratios, we know exactly how many people were vaccinated in these sites — on these days, at these times, and that was the thing that impacted me, seeing the lists of vaccinated at this time, and then five minutes later, and two minutes later, and two minutes later, and then the scatter of delayed deaths. I wasn’t prepared for that, and there’s been no transparency from government about that, and without this sort of data, that would not have been possible.
Winston, your comments on that, as you were amassing this bravely for the world, was that what was hitting you as well?
Yeah, well, I’m looking at the data. That’s the last thing you expect to see. It’s the last thing you want to see. It’s hideous when you look at it, and you realize that these are actually human lives. So when I actually connected the dots and put the dates of death in there, if you were scrolling through the data, ordinarily, you’d see one or two deaths pop up as you’re scrolling through hundreds and hundreds, and that would reflect the underlying mortality rate, but then when you see a whole bunch of them, 10 at a time, 20 at a time, 30 at a time, and then you realize it’s the same vaccination center, and usually the same vaccinator as well, the same person doing it, and then you look at the times between those and you realize that 30 people were all vaccinated within two hours of each other. In a two-hour stretch, and now those people are no longer with us. That’s heart wrenching. That is awful, and the thing is that they don’t all die at the same time. They all die at different times, but people will start to realize there are a lot more people, old people, dying now, and it could be, because of this. Prove me wrong, prove this data wrong.
This crime couldn’t have been revealed as clearly without this data, and that’s why this transparency is so important.
But Paul, what would you say to somebody who looks at it and says, but some of these are in their 80s and 90s, they simply would have died anyway. Give the answer to that from your viewing of the data.
It’s just not possible in the numbers that they have died. We looked at the statistical analysis of this. Yes, elderly people were largely affected, and to me, in some ways, that was reassuring that we weren’t seeing huge numbers of young people, but it’s just the sheer volume. It goes well beyond what you could reasonably expect.
I have looked at data on people under 40, and it is shocking, Paul. I don’t know that you’ve seen those pages because there is such an enormity of data for people in future months and years to get into from this amount of information. There will be proper scientists, ethical scientists studying this, I believe, Winston, for years to come.
Let’s hope so and with real science and not the Fauci-science and that they do actually do a good job of analysis and they’re transparent and truthful. I mean, they should go with science that the Hippocratic oath should follow and that’s ‘First do no harm’ and then do good. We must all abide by that. So if you’re looking at this with an agenda to try and hide what the data shows, then no, you shouldn’t be looking at it at all. You’ve got to look at it with open eyes, and I’m not biased with it. I wish this was not a thing, but these statistics, it’s mathematics at the end of the day, and when you calculate the probabilities, you realize that it’s just off the scale. This vaccine is a killer. We’re talking about a hundred billion to one against it, not being a killer. It’s just unreal.
On that note, let’s get into the first slide then and go through this with you, Dr. Paul. For me, Paul, it was in Winston, a marriage of his absolute understanding of numbers and statistics and mathematics and the importance of those to tell the truth, a marriage of that with his deep humanity, his deep caring. He didn’t just see these as numbers any more than you did. Would you agree with that, Paul?

Yes, absolutely. I mean, this first figure, you’ll notice days when you had deaths of over 120 people, when there were years where this didn’t happen. It’ll show the cross church earthquake. So this figure one goes back to 2012, and you can see the earthquake as one of the lines, and then you can see those blank spaces. That’s whole years… New Zealand’s not such a big country that you expect to see 120 people die in a single day, and each one of those lines is a day that exceeds that number. You can see a flu pandemic. You can see the Christ Church Massacre as a red line, and then look at the clusters of 120 dead per day since the vaccine. You saw some deaths around COVID, but it’s a solid, it’s so many days now, day after day. It’s a tragedy, and this is record-level data, something dramatic has happened, and of course New Zealand, like Australia, was in a unique situation in that it didn’t have a lot of COVID before the rollout.
Why the 120 number here, Winston, just make that clear. The deaths over 120 people per day.
It’s just a number that I came up with to show that how rare it is to have that many people die in one day, and if you look at the chart there on the left, there’s the Christ Church earthquake, which is the outlier, and then there’s nothing 2013, not a single day where you had that many people die. Then 2014 is one or two. Nothing for 2015, 2016. Yeah, very few and far between, and then you get a big hit, a flu epidemic. I think that was July 2017 and then 2019 pretty quiet, and then it starts taking up more or less after the vaccination rollout, which is kind of suspicious.
Thick black, it means so many days are exceeding 120. So as you said, Winston, it’s like many versions of the Christ Church massacre are now happening in New Zealand.
It is absolutely not talked about, not taking anything away from the Christ Church massacre, which was, horrific, but we are seeing an equal number of people dying, and it’s just not being talked about. It’s just nothing. It’s just, oh, yeah, excess mortality. There’s more people died in New Zealand than ever before, and nobody’s talking about it, it’s weird, and this is global as well, it’s not just New Zealand. This is a thing that’s happening in all the countries of the world.
Yes, I think it makes the point that a silent massacre is going on, and this is why it has to be addressed.
Well, this is excess mortality and it does need to be addressed. It does need to be debated, and as, you know, Andrew Bridgen said in the UK Parliament, there might be the first debate about it, but by God, it will not be the last.
For those who say oh, well, those deaths could be due to COVID itself….take us through this.
Yeah, this is the worldometer website, which anyone can look at, and what it shows here is the daily deaths per day from or with COVID in New Zealand.
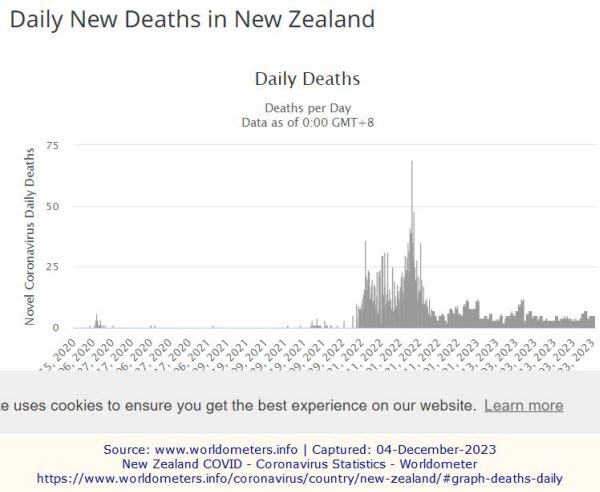
So we have the peak here, that line that sticks right up is July the 30th, 2022, where there were over 60 deaths attributed to COVID, which when you think about it, July is the peak flu season anyway. It’s when most people tend to die off in the middle of winter, and that’s in every country. It’s nothing special about New Zealand, but on this particular day, there was over over 60 who were said to have, succumbed to COVID. So after that, it just drops off. It drops off quite dramatically. I mean, that’s a big peak and a big drop down, and then after that, what we have pretty consistently numbers under under 10 attributed to with or from COVID. So the deaths from COVID are basically that there’s none anymore. Nobody’s dying from COVID.
However, the mortality rate, the death rate is still going up from this point. So if you look at, if you look at that, 2022-23 (in first figure), those thick black lines. So if you just superimpose those two together, the thick black line is happening right after peak COVID.
When in fact, supposed COVID deaths had dropped right away.
Yeah, you see that it’s on the chart that peak deaths from COVID. They’re the black line and there’s still more. It’s still going on.
Take us to this green line to the monthly rate. Explain that.
Well, it’s the way of representing it as a rate, and it’s a little bit compressed there. You can see the lack of deaths on this chart on figure one, you can see it’s basically zero, and then it lifts clear off zero. It’s showing the sustained whack of these 120 days, one after the other, and on figure 3, you can see its relationship to to the vaxathon.

There’s so many lines there that you can’t, you can’t resolve them. So when you zoom in, you can see quite a coincidence there. I say I’m not a conspiracy theorist, I’m a coincidence theorist, and look at the relationship to that vaxathon.
Yeah. So this is the chart from 2020, and as you said, if we look at the monthly one, these are the number of days within that month where you’ve had more than 120 people dying. So if there’s no people, there’s no days over 120, the monthly one will be zero, that green line will be a flat line zero, and then if there are two or three or more days where there’s more than 120 people dying, you’ll get a blip and you’ve got a huge blip here, and just after the vaxathon, that thick black line, those are days and days and days where more than 120 people have died, and it’s way after the vaccine rollout as well. So as you see here, these blue lines, you’ve got the border workers, you’ve got the frontline workers, elderly, and the at risk, and then July 2021, you’ve got the main rollout, and then a vaxathon. So, COVID was over by the stage, but the increased mortality rate wasn’t. It’s only just getting started at this time. So with no COVID, how do you explain the increased mortality?
We also had Omicron, which by then, which greatly reduced the lethality of COVID globally. So it was at a time that COVID wasn’t the killer that it was early on, and it was at a time that coincides with the drive to give this injection.
It’s very sobering to me, even though it is a statistical mathematical and graph represented to me, I also see gravestones. I see families. I can feel that pressure of humans and families torn apart when I look at those lines. They represent so much more than just lines, don’t they?
Yeah, that’s the hard part about looking at this data. As a DBA, you just see letters and numbers. That’s your job. Just a table of rows and columns of data, it’s just meaningless a lot of the time, but when you connect it to a date of death, you realize that someone is sad at this point, someone is hurting, and that’s someone’s mother, grandmother, grandfather, friend, relative, there is sadness here, and it’s increasing, so it’s very hard to look at this without thinking, there is a lot of pain here. There are a lot of people who are looking for closure, and they haven’t got it from the government. They’re just turning a blind eye up until now, and we’re just going to make them open their eyes and see.
And from the government, from the mainstream media, and from the mainstream medical model as well, those outliers like Dr. Paul understand it, but there are still many in our hospitals who are not looking at the truth of what’s been unrolling in front of their eyes.
Yeah, I think on some level, they’re seeing it because we see that in the resolution polls, we’re seeing it in the declining vaccination numbers. Of course, the concern now is the WHO wants to bring in mandates for future pandemics, and we have to look soberly at how we’ve behaved during COVID, and then the result of the response the first time around, it doesn’t give me any confidence that the International Health Regulations that they’re changing and the bringing in of the WHO pandemic treaties. We have to face the carnage of COVID first.
And the WHO pandemic treaties reach across countries boundaries as it were and remove a country’s sovereignty. So it’s extremely dangerous. Not to mention that the WHO is now funded, its primary funder is a corporate, it’s the Gates Foundation, it’s Bill Gates, whose name has not come through this COVID rollout with respect from a vast number of people around the world. He has lost the trust of many people in the world, including me. What would you both say to the people of New Zealand and Australia if they start to be sold a pandemic treaty run by the WHO as being a good idea for our health? What would you say, Dr. Paul, first of all.


I would say that if you didn’t like medical martial law, which they call lockdowns, and if you didn’t like mandates the first time around, it’s time to make sure that politicians know that we have to exit these treaties, that we have to exit the WHO because we’re in danger of it repeating itself, and that’s why it’s so important.
And Winston, your view?
Yeah, totally agree with that, and I’d just like to ask, who elected the WHO? Who are they? The United Nations body, unelected, controlled by corporates, like you say, very shadowy and sinister, and I’m not going to go down any rabbit holes or anything like that, but I just do not like an unelected body having total control over my life, and to tell a government, oh, this is this is how it’s done now. It’s ridiculous, and especially the things like a WEF. I mean, who’s that Schwab? Klaus Schwab, who elected who made him the leader? Who made him, the boss of the world?


He’s literally a Bond villain. You just gotta hear him. I half expect him to say, “I’ve been expecting you, Mr. Bond”. He just oozes evil, and I get very leery of Germans talking about elites and globalism. It didn’t work out too well in 1939, and it’s not going to work out too well now. I’m very, very wary of that organization.


And those are crucial points by you both, but they also raise the specter of medical tyranny, being a doorway to governmental tyranny by the few who are the puppet masters for these paid up politicians. There is a worldwide awakening to this.

Yeah, this time Big Brother came with a stethoscope. So it’s my profession that manifested this tyranny and tore away, as Winston said, ‘do no harm, do good’. It’s torn my professional apart and it’s made it into a device of mass harm, and we have to face up to this, and this is not the only data set that points to it. Ed Dowd talks about it in his book, “Cause Unknown“, the actuaries see it, the insurance industry sees it. It’s present in the excess all-cause mortality, globally. So this is just further confirmation with hard data that it’s real, it’s real, but there are many data points pointing to this, and we have to face up to this, this doctor, this healthcare related harm. (02) Cause Unknown: The Epidemic of Sudden Deaths in 2021 & 2022 https://www.amazon.com.au/Cause-Epidemic-Sudden-Deaths-2021/dp/1510776397
That must really hurt Paul, because you are such an ethical doctor, you are what doctors should be, you really live that edict of ‘first do no harm, do good’. So do you think the medical profession can come back from the crisis in which it finds itself where many doctors have potentially gone along with what they knew from the beginning was at least questionable, if not wrong. Can those doctors be brought back? And if you like, retrained back into an ethical model of medicine?
I think we have to rebuild from scratch. When I did the lighthouse declaration with a couple of my colleagues, Robert Brennan and Ros Nealon-Cook, the psychologist, we were the first, we were early suspendies, but I was the first, but Robert was the second, and Rosalynn was the first psychologist. It was just a call to basic principles. This is the right of informed consent, the end of censorship, I faced a lot of censorship, a lot of the messages that I put out, never made it to the public, because of the sentence. If you don’t have free discourse, you don’t have science, you have an ideology, and you don’t have informed consent, and bodily autonomy is simply medical freedom, and the right to say no to procedures being done on you without your consent, and if we don’t have bodily autonomy, we’re already enslaved. This is why these issues are crucial.
I would go further and say, if we have censorship at all, we cannot have democracy. They’re not bedfellows. One rules out the other. Censorship stops any kind of real democracy in action.
That’s right. I feel like we’re living in 1984. 2020 was 1984, and it’s been 1984 ever since.
Do you hold hope though for the medical profession? Do you think more are waking up now? And do you think this data will wake them up?
I think people are waking up. Look, it has to stop. They’re still giving these shots to children who don’t need them and are being harmed. They’re still given these shots to pregnant women. We know that it has serious contamination issues with Kevin McKernan’s work and now confirmed the multiple sites with the DNA contamination. We’re seeing the cancer clusters and the rising cancers and rising cardiovascular—heart attacks, strokes. We’re seeing the evidence of things that I warned about in 2021, that these shots would produce antibody dependent enhancement or vaccine-linked immunodeficiency, and so it never had any safety studies in pregnancy. It wasn’t studied in in the high risk elderly that we’re seeing dying in this data. It needs to stop. It needs to stop. It needed to stop in 2021, but it’s long overdue that it needs to stop, and that’s what drives me. They’re still giving this to children. They’re still giving it to pregnant women. The government is still recommending these shots. The advisory bodies, which, have been affected by, courted by big pharma and moneyed interest, and it’s leading to untold suffering, and I think that’s what this data shows, that we have to stop.

Was there data Winston on still births? Because Paul raises a very interesting point. I had young friends who were pregnant and I could find no data in the early part of the rollout on breastfeeding—the risks and dangers of that—and certainly no data on the dangers to pregnant women and the risks of still births and miscarriage. Did you come across any of that?
There is no data as far as I’m aware of on that. Difficult question. I can only show you what I can show you, and to go back to Dr. Paul’s point about bodily autonomy. I mean, man, that that is everything to me, and your body is the most precious thing that you’ve got, and you should never, ever be forced to undertake a procedure that you do not want just to keep your job, and when a politician said nobody was forced, that’s an absolute lie. They made you do it, and that just sickening to me. So yes, your body, your body is first, and we need to ratify the Nuremberg accord. We need to look at it again. It’s like, what came out of Nazi Germany after World War II, you should not ever, ever experiment on human beings, and yet what are we doing now? This is crazy. This is absolutely crazy.
There was coercion. It was clear coercion, and say that there was no coercion, and coercion obfuscates, it nullifies and from consent. There’s no way you can say, it’s like the difference between and, nullifying it, and they’re minimizing it. I remember when I used the term bodily autonomy, which is just bodily freedom, the right to say no, my body, my choice. My colleagues sneered, they sneered as if I’ve made up the term, and so that just to answer your question, Liz, is the hope for my profession? I think it has to be rebuilt from the ground up because they’ve lost their moorings totally, and the trust that’s been lost by the public is deserved. It is deserved, and so until they recognize and really look at how far they’ve come away from their ethics, I would say there’s no hope. We have to rebuild, rebuild the healing profession, rebuild the regulators, rethink everything.
I will add in here another whistleblower from a year and a half ago, Dr. Bruce Dooley, who lives in the northern part of the South Island, came forward and told us about something called the FSMB, the Federation of State Medical Boards in Texas, America, which rules all medical councils and medical boards around the world, and it became very clear in that interview, they are like the enforcement arm for big pharmaceuticals, and FSMB was set up in 1913 by Rockefeller influence. Now, I’ll attach that interview for people who haven’t seen that, but it shows that our medical councils are absolutely fallen around the world, and Joan Simeon, the head of the New Zealand Medical Council, heads the international arm of the FSMB, which shows that New Zealand has been focused on. This leads into the idea that we are some kind of petri dish experimental nation. (03) Explosive Interview: Dr. Dooley and The Smoking Gunn https://nzdsos.com/2022/09/28/explosive-interview-dr-dooley-smoking-gunn/ (04) FSMB https://www.fsmb.org/
Let’s move on now, Winston, to the next slide, and see just how this experiment has played out in this country.

The 20 worst sites for excess deaths. So this is a ratio of mortality rates, and if you look at the map, you will see something which jumps out, bearing in mind, one in three New Zealanders live in Auckland. There is something very unusual about that map. What it’s showing is these are sites where there are clusters and a high ratio of deaths per site, and if you look at Auckland, there’s only one or two, and yet, on the South Island, there’s masses of them. The most deaths are occurring on the South Island per capita. You’ve got to wonder why, what is happening here? It’s a mind-blowing thing. Auckland is relatively unscathed. Yet, Christchurch, Invercargill, and places like Gore got absolutely slammed.
What jumps out at you, Dr. Paul, on this map?
Well, I wouldn’t want to be in the South Island. It makes the point that there is some serious problem with the way this rollout was conducted. You would expect that the deaths would be evenly distributed and would be higher in the high population areas, and we’re seeing areas that are more remote, that are facing incredibly high rates of death proportionately, and so that’s a problem, and we can speculate as to the cause of what led to this distribution, whether it was an effect of batches, whether it was effective storage and handling, but this shows that we have deadly batches, and they’re being distributed largely in the South Island of New Zealand.
10 of the top 20 are in Christchurch alone.
Aas Dr. Paul said, it is not a populous area. There are far fewer people down there. So on the left there, we can see the total sites for jabbing New Zealanders. There were 1,391, and then a cluster, Winston, just to explain what a cluster means.
Well, what I defined as a cluster as is a group of three or more in a row of people who died from an injection. So you could be injected within a couple of minutes of each other, on a certain day, at a certain time, by a certain person. If you are no longer with us, and there’s a group of three or more, then that’s a cluster.
Those are 471. We have 471 clusters.
So when you look at places like Auckland, there’s only only a couple of sites in Auckland. 30% of the population of New Zealand live there. So yeah, there’s definitely questions that need to be asked about this. So you see most of the South Island, you get nothing. The big population centers…
Most of the North Island.
Palmerston, New Plymouth.
That doesn’t mean there weren’t deaths there. It means they are not in the top 20 clusters.
Exactly right, but then when you go to South, you go to Christchurch and you start zooming in, oh my God, look at all those crosses. 10 of the top 20, and then when you go down, Ashburn, not a big place,
These are all the hotspots.
Yes, these are all in the top 20, and remote areas. I mean, for goodness’ sake, you’ve got to ask questions, how come, how come? I think Invercargill was the worst of the lot, and places like Gore, Gore had two sites in the top 20. A little place like Gore,
And Gore has a tiny population. To have two sites with excess deaths.
Yes. It’s 0.02% of the population. So it’s a very small population. Yeah. Invercargill, I can’t get it now, but there’s one site called the Queen’s Outreach One, and it’s got a cluster of 51. So I mean, 51 people died and they’re all within two hours of each other, and it’s unbelievable, and it’s like, this should be an inquiry. It’s like, what exactly happened on that day to cause this? Because 51 people dying who were all injected at the same time. They didn’t all die at the same time, but they were all injected at the same time. Now, no longer with us, you’ve got to ask some questions about that. It’s like you’re sitting on a bus with a group of people, and you’re one of 51 on the bus, and then a year later, you are the only one that survived out of the whole bus. It’s like the chances, the chances of that are so remote. It’s almost impossible. That’s what a statistician would say, almost impossible, but the real odds are trillions to one against. So that basically points to if it’s nothing else, Occam’s razor, when you eliminate all of the factors, what are you left with? What is the fundamental underlying cause of this? And the only thing that is left logically and scientifically, is the vaccine itself. There’s no other cause.
And we’ve been told it’s climate change. It’s going to sleep in front of the television.
It’s every sort of ridiculous coincidence, and the thing that’s unique about this data set is, I think it should show anyone that this is an unsafe product that had multiple, multiple bad batches that led to unnecessary deaths, and there’s no way it could have happened if it was safe.

Let’s from both of you before we move from this slide. There’s one country and the data, is from this one country. Now put it in the context of its relevance to other countries around the world. I want your views on how important this data set Dr. Paul is in your mind for showing other countries what may be going on there, even though they may not yet have the data set that we now have thanks to this brave whistleblower.
It’s not isolated to New Zealand. This is this is a phenomenon which is is doubtless happening all around the world, wherever these products have been used, and as more whistleblowers come forward with record level data, we will see it, and this is the thing, it’s been hidden. My initial thought was, you have a date of vaccination and you’d expect the deaths to happen, and certainly a lot do happen early and within the first two weeks, but what was the surprise was all these delayed deaths, and there’s no way, if you didn’t know that they’d all got the shot in a particular place on a particular day with a particular batch, there’s no way you would have seen this. So hat’s off to Winston for this, because it makes the point very clear that we need inquiries. We need to stop the shot.
We need multiple inquiries in every country around the world now. Winston, what is your desire? What is your wish to come from this crucial data?
Yeah, lots of things really. I want more whistleblowers to come forward, definitely. This is a thing. There are other databases around the world. New Zealand isn’t the only system in place where we have this data. It’s everywhere. It’ll be in all Western countries. They will have this data. They just have to be brave enough to get it out and show the people, and yeah, let’s have a debate about it. Let’s have an open discussion. Prove the data wrong. We’re all open. We’re all up for criticism, whatever. Bring it on. Show us where we’re wrong with the data. What is it we’re missing? How does this fit into the norm when you’re looking at 100 billion to one chance? Is that normal? No, not when there’s only 2.2 million people in New Zealand, and it would take one vaccinator 38 years vaccinating 24//7 nonstop to come up with a similar size data set on a cluster of 10, not 51… 10. So the chances of it not being this impossible.
Just a correction there. This database contains 2.2 million New Zealanders, but there are 5.3 million in New Zealand. That’s the population.
5.2 something at the last count that I saw that’s on another slide, but yes, this is not the only system in the ministry that I work for. It is probably the biggest, but it’s a system that I was involved with right from the beginning. I helped build it, implement it, wrote some of it, supported it. So I know this data. I know this data.
Can you tell us a bit more about the system that you built because other countries, let’s hope, that other politicians in other countries will stand up like Andrew Bridgen and demand inquiries and then use this sort of entry point. What was this data about?
The unique thing about this data is it is a payment system, basically, and we pay for each dose that is administered by the providers, the health care providers. So they set up these vaccination centers. They perform a lot of vaccines. They record all this data in amazing detail, by the way. It’s all high tech stuff. So even the time when the needle goes into the arms recorded, when the needle comes out of the arm is also recorded. So vast amounts of highly accurate quality data is encapsulated in this system, and it’s for every single dose that is administered, the providers get a payment, 35 dollars or 40 dollars dependent on if it’s after hours or public holidays, things like that.
I’ve heard $60, $100, a wide variety of money making.
Yeah, there is a financial incentive definitely for this. So you think, if you’re a provider and you’re getting paid 40 bucks a shot, what is it in your best interest to do? First, do no harm? I’ll just get those needles in as many arms as possible and get the money.
That’s the thing about this, the unique thing about this data, just how much information is there. Up to now we’ve been positing this data from murky data sets and putting it and we now virtually know what the person had for breakfast. it’s the high level of data. we know the date of birth. It’s incredible, and that’s why I think it’s going to be a great resource for finding out what went wrong and why it’s just so incredibly powerful and makes the point that this shot has to stop.
We won’t say their names yet because they’ve asked us to keep them private, but you have sent this started to overseas statisticians as well haven’t you?
Yeah, well, I’m not a statistician by trade. I’m not a data analyst. I do know a bit of maths. I’ve got a scientific background. I know computers a lot. Know database’s a lot, but yes, to get some validation, it’s easy enough to send over a set of redacted data. You don’t have to mention names. You can redact the sites, even you just say it’s, site A, site B, that sort of thing. vaccinator 1 vaccinator 2, that sort of thing. You can hide all the identities you want, and you keep, a data birth, which gives you an edge, and you can then do all sorts of analysis at that stage. It just becomes data. It’s just a question of doing some statistics on it. So you send over this data, and yeah, people will look at it and say, well, this is statistically significant. This cluster here, this should never happen in the size of the data set. 2.2 million is the number of individuals who have been on this system. I think that the total number of vaccinations per se that this our transactions is over 4 million, but 2.2 million actual people on the system, and from that, you can extrapolate all sorts of stuff when you’re looking at stats. It’s just purely a stats exercise and you say, well, if this is the underlying mortality rate for this age group of people, then the chances of this cluster here happening almost zero, and that’s just one example. there’s multiple clusters. There’s clusters everywhere. There’s clusters of 10, 20, 30, 40. So when you add all that together, you’re looking at an impossible event.
There’s some amazing information in here, and I cannot get all of it out. It would take me a lifetime to do that. So that’s why I’m relying on people from, universities, academics, whatever, have a look at it. Just look at the redacted data and just see it as a statistical exercise. You don’t have to mention, these are people, just have like two dates and say, what are the chances that this happens? What comes out of this will will be interesting. I mean, it’s already mind blowing stuff, right? But there’s a lot of data in here to unpack. We’re only just at the start of it, and this is just one place in the world, and hopefully it’ll come out that there are other places with similar data that they can share.
Your heroism will inspire others.
Let’s hope that it comes out, because people need to know. These are human beings. These are people’s lives.
What is a P number that you referred to before?
Well, in statistics, you can never say that something is a hundred percent certain or impossible. It’s always couched in terms of probability, where zero, you’re approaching zero, which is impossible, or approaching one, which is certain, and some of these P values have got such large negative exponents, such tiny fractions that there was close to zero as I’ve ever seen. just incredible. If this was safe, if there weren’t clusters, if this wasn’t a real event, you wouldn’t be seeing these sort of numbers.
So P value just briefly is?
So it’s a probability. It’s a probability. So like in a study, you might say, this effect is real if the P value is 0.05, which means that 5% that this result appeared by chance, or 0.01 or 1% chance. So if you did a hundred studies, maybe this result would happen in one of the studies. Now we’ve got 0.000000000000. So many zeros that, in the world of probability, it’s as close to impossible as you can get, but it’s always couched in those terms, in terms of statistics.
Impossible that it would be caused by a natural event?
By chance.
All right, let’s move on to the next slide. This is very helpful.
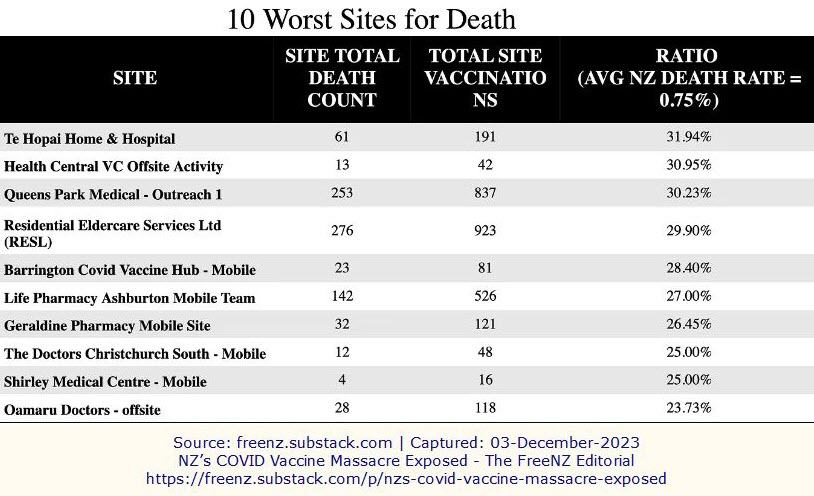
These are the top sites, and it’s got the number of deaths within that site and the total number of vaccinations and then the ratio. So we just divide one by the other, come up with the ratio, which is percent, and the underline average mortality rate for New Zealand, 0.75%, just bear that in mind. So what we see here, these places, these vaccination sites, we have the top one there, top of the chart, 31% mortality, nearly 32%. So it means almost one in three people who went to this place or were in this place, are no longer with us.
They were in this place and they received the vaccinations and a third of them died.
Yeah. Now they’re gone. The other one, 30%, 30%, 29%, 28%. These are huge mortality rates, absolutely huge, and the other thing that we talked about, the South Island, but we didn’t mention is that nearly all of these sites, all of these sites are mobile sites, which is another question that needs to be asked. What is happening with the mobile sites? Why so many deaths from mobile sites?
Explain what’s your definition of mobile?
They go around to rest homes, nursing homes, schools, places like that, with the COVID vaccine in a truck. It’s got to be specially treated and handled and all, there’s a whole protocol around it. So they go to all these retirement villages and whatnot, and they will just then go and inject, vaccinate all the residents there.
And look at the numbers, Queens Park Medical, 837 vaccinations, 253 of those are not with us anymore.
It’s horrifying. These are these are questions that need to be asked. And, I’ve said it before, we shouldn’t shoot down, we need to shoot up (past) these places. We’ve got to look at who is responsible for this at the end of the day. We need to point upwards. It’s the politicians who mandated it. It’s the drug companies themselves that made it and never did any proper tests on it. Those are the ones who are really responsible. It’s not the sites themselves per se.
I know that there’s an army of trolls and paid workers who constantly argue whenever you raise a safety issue or an issue of corruption, there’s a vast army of paid people to pay cover for it. This is why, you just look at this and you can see that it’s not going to be easy to cover this. It’s not to single out these sites, but just to make the point that this will not be easy to cover.
No, you can’t. These these mortality rates are off the charts. So they can’t be explained under normal circumstances. So they have to be held to account, and these people who have these jobs to say “everything’s normal., nothing to see here, move along, move along.” It must absolutely suck to be them. I feel so bad for them to have that kind of attitude and that kind of life. At the very least, they’re complicit to it, and if they know what’s really going on, and yet still the narrative that they give is to take the vaccine, if they know in their heart that it is a killer, and yet they’re still telling people to take the vaccine, Oh, shame on you.
Shame on them, and one thing I would want to come out of this interview is this: Please, if you are watching this, can you send it and send it and vast numbers to your local newspaper, your national newspapers in mainstream media, and demand that they look at this unequivocal data so that they will no longer hold up the government lies and the government and pharmaceutical misleading information that we were given from them. I would ask you to demand of your mainstream media outlets that they start telling the people the truth. Let’s move on to the next slide, Winston.
Yep, good luck with that, by the way. So these are the batch numbers that we have.
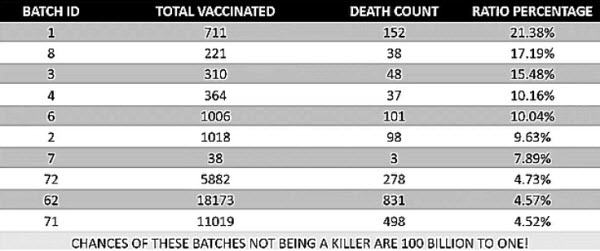
We don’t have the actual Pfizer batch numbers, but we can, we could get that from official information requests. I’m sure people are entitled to know which batch of the vaccine that they were injected with, that should be a fundamental right of information that we all have. So we’ve got our internal system batch IDs, which do correlate to the actual Pfizer batch IDs. So you’ve got the batch ID, you’ve got the total vaccinated and total death count and the ratio is similar format to before. So you see from batch ID number one, you’ve got 711 who were vaccinated and 152 of those are unfortunately now dead, which gives you a ratio of 21.38%. So it’s one and five who were vaccinated by batch number one, now no longer with us.
Can you take us through the next few lines there?
So the batches were rolled out sequentially in time order. So you would expect the earliest batches to have the highest death count just because they were the first ones rolled out, and it’s also those are the batches that are going to be dose number one and dose number two, because everyone was dosed up with the first batches, right? So after that, the higher the batch number, the higher the dose number. So it’s basically the correlation is the lower the batch ID, the lower is the dose number that is going to kill you, if that makes sense. So if it was a sequential thing, it would be like one, two, three, four, five, but it’s not. You get a batch number eight. Batch number two is in the middle there somewhere, three is there. Five isn’t even on there.
Could we go through batch 8? So you have 221 total vaccinated. You have 38 dead. That gives a ratio of what?
17%, and bearing in mind that underlying mortality rate 0.75, and these batches, they’re administered across the board. There’s no specific age range to them. So they should reflect the general New Zealand population, and if they reflect the general New Zealand population across all ages, then the mortality rate should be 0.75.
Wow, and instead for batch 3, we’ve got what ratio there?
15.48%
And I think the key line here, Dr. Paul, is that line down the bottom. Could you just read that out?
Chances are these batches not being a killer are 100 billion to one.
Wow.
I got that from one of the world’s leading statisticians.. So it’s verified. It’s not me. I didn’t say that. He looked at the data and said, this is not a chance.
So it’s not one batch. It’s not one batch. It’s batch after batch after batch after batch. That’s how you get to these ridiculously unlikely results.
I mean, 100 billion to one, 2.2 million people in the system. there’s not 100 billion people in New Zealand or even the world. These are crazy numbers.
100 billion to one means you’d have to inject 100 billion to get these results.
These results. Yeah.
This is crazy. Paul your reaction to this. Your medical background, it must be shuddering.
Yeah. I mean, these ratios are incredibly high. and yet we’re still echoes of ‘safe and effective’, ‘safe and effective’, ‘safe and effective’. There is no way that these can be safe and effective when they have batch after batch after batch, which is killing such a high proportion of the people who have received them, and people should be very, very concerned and should demand that it stop.
Absolutely, and beyond that, demand that those who roll this out, particularly if they knew this, even if they didn’t, they were negligent not to know this. Those in government who kept insisting on this, need to be held accountable in our courts of law, in my opinion. What do either of you say to that?
I agree. Accountability is something that I’ve been talking about since 2021. That’s what I warned the then Health Minister. This is why I’m so grateful for this data. It’s time for accountability and it’s time for it to stop.
Let’s move on to the next slide, Winston.
Just to echo, I’m totally 100% in favor of that. The people do need to be held accountable, and the people need to see that. There needs to be, just needs to be done. So we will get there.
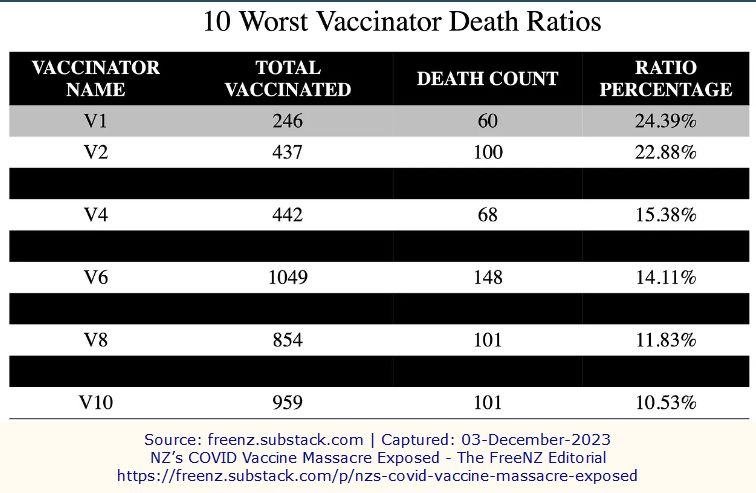
This slide is a vaccinator names. So I’ve redacted the names of the vaccinators. These are the top ones, and you see vaccinator one there, they jabbed 246 people. 60 of them are now no longer with us. That’s a percentage of 24.39%. That means one in four that they injected died, 1 in 4. That’s like Russian roulette with a revolver, but only four chambers, one in four, and moving down the second highest, 22%, close to one in five, and on and on it goes, it’s just, and these are big numbers as well. This is not, this is not a statistical anomaly. If the higher the number you get, if the numbers over 200, you can, you can discount skews. Vaccinator 5 = 1682 vaccinated, 239 dead. 14.21%. A huge ratio. This might be related to sites and batches. There’s like a ton of work that needs to be done on this, but there’s a ton of questions that need to be asked.
Will you be putting this redacted data out for the world’s population to see, or at this stage, are you going to focus on the scientists and the statisticians?
Yeah, I’ll give it to the scientists and statisticians first, just so that it’s protecting those involved as much as possible at this stage. Just so it’s an exercise in statistics. It’s got to be seen that way, and then there’s no bias involved.
I would advocate in the end for it to go wider than that, because there are many very astute people who have sorted out a lot of information for themselves in the last few years. It’s incredible the number of self educated and very awake, very aware human beings around the world now who’ve had to analyze and work out through the mountain of lies they’ve been given what truth is.
Absolutely. This is government data. It’s 100% accurate as far as I can tell, and so they cannot deny that this data exists. It is your data. And it needs to be analyzed to the nth degree so that we can get as much out of this as possible and then make sure that we never go through this hell ever again.
So in the long run, would you put it out to the wider population, Winston? Would you consider that?
Yeah, absolutely. Yeah. It’s the public’s data. It’s there for their consumption. I just want t to be seen by all the Harvard people, the Oxford people first, so that they can get a clear, clear shot of it.
I’d love Jay Bhattacharya from Stanford to have a look at it too.
Stanford. Yeah, absolutely.
Population breakdown by location. So I focused just on Auckland, Christchurch, Invercargill and Gore, because that was like the total, the skew of the South Island with Gore having two sites of interest, and Invercargill, having the biggest one in Christchurch, having over half of them. So if you look at it normally, the population, how it breaks down by each population center would look like this. So if you’ve got Auckland here, you’ve got your population, 1.6 million, which is basically one in three of New Zealanders live in Auckland, Christchurch population, 7.7%, then you’ve got Invercargill, 1.1 Gore, right at the bottom, 0.2% of the population of New Zealand live in Gore, and the rest of New Zealand is 59%. So that’s just basically a population breakdown, the most current stats I could find.
The next one, what we’re looking at, is the distribution of the top 20 worst sites would be under normal population distribution. So on the left hand side, if it was a normal sort of thing, you’d see Auckland sites, you’d have between 6 and 7, just because of the size of Auckland, they’re a bigger city, Christchurch, you’d have between 1 and 2 sites in the top 20. Invercargill, you’d have 0, essentially, 0.22, and Gore sites, forget it, Gore should not be on this, and the rest of New Zealand should have between 11 and 12 sites of interest, but what the actual data shows, you’ve got the actual distribution of the top 20 worst sites, Christchurch, over half. Now compare that to the left hand side, Christchurch has got 10 sites, which are in the top 20 alone. The rest of New Zealand, you’ve got five. Auckland, you only have two, bigger city, only two sites of interest. The same as Gore, Gore 0.2% of the population. With two sites, the same number as Auckland! Questions.
Invercargill, you’ve got the worst of the lot, the worst cluster of the lot, 50 people injected within a couple of hours, now no longer with us.
That is extraordinary, and I think Gore has only about 13,000 people, and look at its representation there. What is this telling us? This is what we just don’t know yet, but were, as you said, Dr Paul earlier, were dirty batches sent down there, were wrong batches, experimental batches. Was it poorly handled? We just don’t know what this is actually throwing up, do we?
No, but we’re seeing lightning striking in places like Gore, lightning that just can’t be explained.
This tragedy is unfolding down there. The people in Gore and Invercargill are probably just asking, what is happening here? They’ve been devastated. They must know what’s going on.
And the worst thing is they’ve been gaslit by the politicians and by their doctors and being told, everything’s fine here. There’s nothing to see. Come and get your next shot, and there is something to see here.
Absolutely, there is.
So, what would you say should be done about this? We need this to be front and centre in the inquiry, don’t we?
Yeah, absolutely. I think we definitely need a government inquiry about this. There’s a lot of questions need to be asked. A lot of questions. I can think of a few off the top of my head. How is it transported down there? Why is Auckland different? I mean, it’s an arduous journey down to places like Gore on the South Island. What were the storage facilities like? because this vaccine has to be handled extremely carefully. I mean, even Pfizer give a whole list of instructions that you cannot store it out of this temperature range, and if you do, you can only use it for how long and it’s unbelievably delicate how this vaccine is. if you go outside any of those parameters, you don’t know what you’re dealing with. If the vaccine is stored at room temperature for a certain length of time they say it’s unusable, but what would happen if you actually did use it?
But Winston, you looked up temperature care for the vaccines. Tell us about that.
Well, anyone can do it. Just do a Google search on the Pfizer COVID vaccine temperatures, and you’ll get a whole list of all government and official websites. All over the world, MedSafe, NIH. The New Zealand ones, British ones, and they will all say different things. They all say different things, how it should be stored and how it should be handled, and for how long. It’s, yeah.
This was a novel technology.
In each country, it’s got to be handled differently. That’s a bit weird, isn’t it? It is strange.
It’s unlike anything we previously called a vaccine. It’s one of the things I told the medical council in my hearing in 2021. That it’s been called a vaccine, but this is a totally new technology, and as a totally new technology, we have no long term safety data, and the lipid nanoparticles also, the storage is vitally important for them because they can clump, and they can behave very differently if they’re not handled just so, and I think we may be seeing evidence of how important that it was handled just so, and yet they went ahead and treated it as if it was an understood known commonplace technology. No, it was an entirely novel technology that had never been unleashed on a large scale. It raises serious questions.
Absolutely and beyond that, I think, at the other end of the spectrum from the poor handling potentially of the vaccine. One has to ask the bigger questions. Was this a form of a hit on the South Island of New Zealand? Was there some experiment on different parts of New Zealand with different dosages being carried out? There are many Kiwis now who are wondering, as I said earlier, if we are not deemed an experimental population by people like those who run the WHO and the WEF and the UN, and there are many Kiwis pushing back on this now. Any comments on that from either of you. These are things that as yet we cannot prove of course.
Yeah, it’s more like the WTF isn’t it at the stage and they’re all perfectly valid questions, and yeah, the people on the South Island deserve answers because this is a terrible, terrible thing that’s happened to them.
This is like a second earthquake in Christchurch. It’s terrible. They’ve suffered enough.
They’ve suffered enough, and we all have suffered enough in New Zealand, in Australia and around the world.
So your final thoughts from both of you. It’s been such an honour to talk to you both, and it’s been really enlightening. This calm way of unpacking, in fact, devastating information, I think will help a lot of people come to terms with what is just so unpalatable in the end, but your final comments, Dr. Paul, from this whole experience of being involved with the whistleblower and his courage.
It’s very humbling to be involved in this project as difficult as it is to see this material. I think we all want people to be safe and to be free, and only by transparency and openness, will we be able to achieve that. Only by eliminating censorship, will we return to democracy. Because I think we’ve strayed too far, and I’m sure we all pray that the benefit will come from this and that the harm will stop, and we will come back to a sane, rational society.
Beautifully said, and your thoughts, Winston.
Yeah, that was amazing. Dr. Paul, thank you. I think we’ve strayed from a road and within a dark, we’re in a dark place now. The further down this road, we go, the harder it’s going to be to get back to where we should be, and we need to do exactly what you say. We need to reassess and we need to change the way we’ve been doing things. This has been a nightmare. The last two years have been an absolute nightmare. It has been like going through Orwell’s 1984. It’s like living a novel. It’s a fiction, but it’s real, and it’s like, these things shouldn’t happen – mandates, lockdowns, and forced. To go on holiday you had to be injected, and the whole Orwellian doublethink. It’s like, this is not true because we tell you that it’s not true. The Ministry of Truth. the Prime Minister saying that we are the single source of the truth. No, you’re not. Come on, and the whole thing about science. “We are the science”, the speed of science. Now, science is science is science. It’s about being skeptical and curious and just wondering about the earth and being open to have discussion, freedom of speech. I might disagree. You might disagree with me. I would die in a hell to protect your right to say whatever you want to say. If you want to get injected 50 times, haven’t seen all the data, then, yeah, sure, go ahead. But I have a right not to do that, and you should respect my right as I respect yours. So what I want out of this in a nutshell is just two words, and I’ve said that right from the start. Never again. Never again this happens. Not for my kids. Not for anyone’s kids. This is just. No, it stops now.
That’s extraordinary. I think my final words to both of you, as a woman wanting to see a better world for my children’s children. You two men give me great hope. We have needed male leadership. Many women stood up at the beginning and spoke out. To see the courage of both of you, to see the willingness to stand up and take whatever comes at you and tell the truth anyway is what we need in this world, and I’m going to reinforce what Winston asked: “Please would more whistleblowers come forward and do what both of these men have done”. But both of you, you Paul as a doctor and you Winston for your sheer courage and honesty, you give me great hope for a far better world to come. Thank you both.
It’ll come. Thank you.
Posts tagged Liz Gunn

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:


References[+]
| 01 | The Medical Board of NSW didn’t mention my Tweet’s to the Minister of Health https://pauloosterhuis.substack.com/p/the-medical-board-of-nsw-didnt-mention |
|---|---|
| 02 | Cause Unknown: The Epidemic of Sudden Deaths in 2021 & 2022 https://www.amazon.com.au/Cause-Epidemic-Sudden-Deaths-2021/dp/1510776397 |
| 03 | Explosive Interview: Dr. Dooley and The Smoking Gunn https://nzdsos.com/2022/09/28/explosive-interview-dr-dooley-smoking-gunn/ |
| 04 | FSMB https://www.fsmb.org/ |
Truth-seeker, ever-questioning, ever-learning, ever-researching, ever delving further and deeper, ever trying to 'figure it out'. This site is a legacy of sorts, a place to collect thoughts, notes, book summaries, & random points of interests.
DISCLAIMER: The information on this website is not medical science or medical advice. I do not have any medical training aside from my own research and interest in this area. The information I publish is not intended to diagnose, treat, cure or prevent any disease, disorder, pain, injury, deformity, or physical or mental condition. I just report my own results, understanding & research.