Dr John Campbell on Australian Senators Ralph Babet & Gerard Rennick

Dr. John Campbell comments on two recent Senate sessions in the Australian Parliament from Senators Ralph Babet and Gerard Rennick on the 20,000 excess Australian deaths and the dishonesty and lack of transparency with the jabs and jab studies (or lack thereof).
21 Feb 2023 | Rumble-Mirror | Telegram-Mirror
Original Sources: Dr. John Campbell YouTube | Senator Babet Speech | Senator Rennick Speech
Other clips inserted into Dr. John Campbell’s talk:
- YouTube Karl Stefanovic Clip “I’ve had covid a couple of times and I’m done with the vaccines… I’m concerned if I have another dose, that I may get complications… fit & healthy people dropping down with heart issues and it’s still not established yet whether or not the vaccine caused some of these heart issues, but that’s a worry for me, more so than getting covid.” (01) (02) (03)
- Telegram [COVID-19 Accountability Hearing] Dr Jay Bhattacharya “If you have a vaccine, that doesn’t stop transmission, you can’t use it to get herd immunity”.
- Rumble Dr Brian Ardis on Remdesivir – the only NIH-approved Covid-19 treatment, “Causes” Kidney failure, Liver failure, and Heart failure. (See also: Post on Remdesivir, and post on Paxlovid)
- Telegram Senator Alex Antic on Pfizer’s EU Parliament admission that they never tested for preventing transmission.
- Telegram EU Parliament Covid Hearing with Pfizer Exec, Janine Small, “We never tested for Transmission” (See also: Post with Full Hearing and more clips)
- Telegram EU Parliament Press Conference with MEP Christine Anderson (Germany) and other Parliament members from Italy, Romania, France, and Croatia: “The cat is out of the bag – it was a gigantic lie – all of the mandates, lockdowns, wearing masks, stay at home curfews, all of that – was based on a gigantic lie”
- Telegram TGA, Prof John Skerritt admission: “I need to emphasize, the vaccines have not been approved for an impact on transmission.”
- Telegram Two prominent Cardiologists, Dr. Aseem Malhotra & Dr. Peter McCullough with an urgent warning that the “excess sudden adult death syndrome & heart-related issues should be correlated to vaccines until proven otherwise.”
Dr. John Campbell: Welcome to today’s talk, the 21st of February. Today I want to play you a couple of clips from the Australian Senate where it’s good to see that questions are being asked about various contemporary aspects of health and public health and, indeed, individual health.
The first clip is from Senator Ralph Babet, senator for Victoria. His video is entitled “I asked the government about excess mortality.” So, over to Senator Ralph Babet:
Senator Ralph Babet: “My question is to the minister representing the health minister, Minister Gallagher. Minister, in November 2022, I raised with you the issue of excess mortality as reported by the Australian Bureau of Statistics.
Now, the most recent full report from the ABS shows that for the first nine months of 2022, there were nearly 20,000 excess deaths, which is about 16% more than the baseline average.
Of those, 8,160 deaths were attributed to COVID-19. So, where’s the rest from? Now, Minister, can you please confirm if the Department of Health has investigated this large increase in excess mortality, and if they have, can you advise the Senate what is causing this spike in deaths?”

(See Dec 2022 post 18% Excess Mortality In Australia Is A Disaster But Media Is Silent, May 2022 post Excess All-Cause Mortality (AU, NZ, UK, USA, CAN), and Jan 2022 post [Rant] More Vaccinated Than Unvaccinated Deaths In Australia)
ALP Minister Katy Gallagher: Thank you. I thank Senator Babet for the question and also for the advance indication that he would be asking a question around excess deaths. I can say that the Department of Health, would as routine, would look at the reports that come out through the ABS.
As the senator indicated in this question, the reports that the ABS does into mortality statistics, the reports they do on the causes of death, and of course, the Department of Health would look at those and examine those to see if there are any trends or issues of concern.
I think I’m advised that it’s important to note that increases in deaths from a range of other causes not related to COVID-19 because there is an indication of excess deaths related to COVID-19 have also been observed in 2022, and examples include death due to dementia, including Alzheimer’s disease, which were 25.6% above the baseline average in June, and 21.8% above the baseline average for the year to June.
And while the number of COVID-19 cases and associated deaths has increased in 2022, I think it is important to understand that the proportion of COVID-19-associated deaths relative to the numbers of cases of COVID-19 has decreased overall, which highlights the positive impact of the health measures, the changes in transmission, the vaccination, and the reduced severity of the Omicron variant and subvariants when compared to earlier COVID-19 variants such as Delta. Thank you, Minister.”
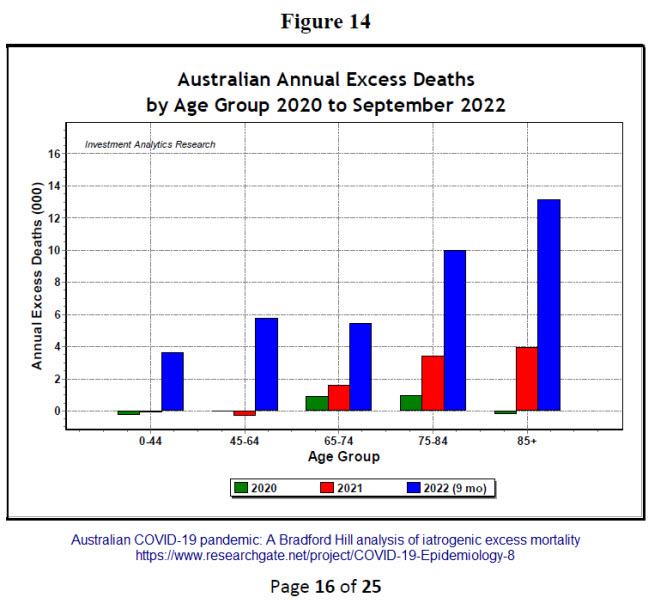

(Feb 2023 – Australian COVID-19 pandemic: A Bradford Hill analysis of iatrogenic excess mortality.
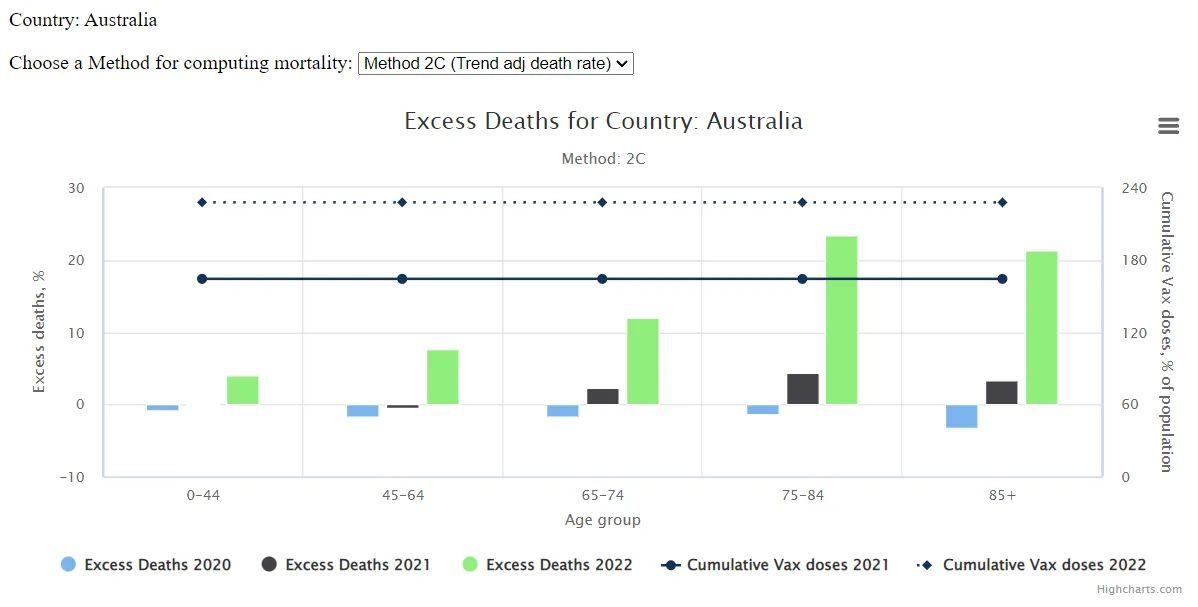
Graph 1: In the nine months of 2022, the over 75 age groups, accounted for 23,086 excess deaths which is 61% of the total 37,934 excess deaths for all age groups. The evidence contradicts the often-made claim that the COVID injections are particularly beneficial to the elderly and the most vulnerable. There was limited scientific basis to the claim, because there were few old participants in “vaccine” trials, e.g., the Pfizer trials had only 4.5% over 75- year-olds, under-representing the demographic. Between 2021 and September 2022 during the period of widespread injections, the oldest 85+ age group substantially increased their total excess mortality by 17,098, while the 75- 84 age group increased by 13,389. The most vulnerable groups have accounted for 65% of the surges in total excess deaths with the advent of COVID injections. The vulnerable, already with ill-health and chronic inflammation, succumbed easily to the added challenge introduced by the pathogens of the injections. However, due to comorbidities of the elderly, all sorts of explanations other than the “vaccines” have been advanced, including “long COVID”, heat waves, climate change etc., for the surge in excess deaths.
Graph 2: What is highly statistically significant is the youngest 0-44 group, with their excess mortality in 2022 was about 160% above historical expectation compared to normally less than 20% fluctuations for all age groups before 2022; proportionately, the harm suffered by the youngest age group has been very high.) (04)
“Now, you mentioned some causes of death there, but you didn’t mention myocarditis and pericarditis. Now, this is an issue which is now in the mainstream media. Even Karl Stefanovic talked about it on Channel 9 recently. He said he wouldn’t take more than two jabs because he had concerns relating to heart issues. Now, Minister, is the government confident that none of this is because of the mRNA injection?“
“President, I thank, Senator, for this supplementary, and I would say that COVID-19 as a virus also impacts health and has those health consequences, so pericarditis, myocarditis, is also, if you have a bad case, a severe case of COVID-19, that is a side effect, a consequence of that. And I would also say that the data shows that for those who are unvaccinated, so haven’t had a vaccine, primarily an mRNA vaccine, they are much more likely to end up are much more likely to end up in ICU or passing away. So, those who are not vaccinated or not up to date with their vaccinations, and for people in my age group, it’s 32 times more likely to end up in the hospital if you’re not vaccinated. So the answer to the question is yes, we are confident that the government and the approving authorities are evident that the mRNA vaccine is safe.
Senator Babet, second supplementary: Thank you, President. Now, Minister, given that you’re so confident that mRNA is so safe and effective, when is the government going to release the data to support this claim? When are you going to talk to a target and tell them to give us the information? Are you going to do this, Minister?
Thank you, Senator Babet. The safety of the vaccine is while the target has a role about the provision of the vaccine, who should be provided the dose, the approving authorities, the TGA, and they do publish adverse events through quite frequent reporting. I think it’s either weekly or monthly reporting of adverse events relating to vaccination status. I would also say that, of course, people are entitled to get advice from their health professional about whether their vaccine is safe for them and take that advice. But I would also urge people with the fifth dose becoming available to please remain up to date with your vaccinations. It’s not just an individual decision. This is the thing. It’s not just about an individual’s decision in keeping yourself safe. It’s keeping other people safe from these vaccines from this virus, people who aren’t able to be as protected as some of us. So it’s actually a community responsibility to be vaccinated.
!
The questions were answered by Katie Gallagher, who was a health minister. There is no question that there have been excess deaths, partly due to COVID, but the majority were not due to COVID. The minister is confident that cases of myocarditis and pericarditis are not caused by the vaccine. But then the minister said that it is a community responsibility to take the vaccine. Not taking the vaccine keeps others safe. I struggled really with the credulity that she said that. Is she actually still saying that vaccines are going to protect other people from infection? If the vaccines prevented massive surges in the Omicron wave, it really is quite surprising to see a health minister saying basically, “get vaccinated to protect other people.” We know that this doesn’t work, but she was confident about the first point.
Now, the next clip we’re going to hear is actually from last year, from August last year, to be precise. The Ralph Babet one was just a few days ago. This is from Senator Gerard Renick, Queensland, and his clip is entitled “What Pfizer and the TGA didn’t tell you.” So, over to Senator Gerard Renick now, and as you’ll hear, he’s certainly done his homework.
Senator Gerard Rennick: Thank you Acting Deputy President. Today, of course, is 2 August, and for well over a year we’ve had the vaccine rollout. Every day I still hear from people that have suffered injuries from the vaccine or suffer through mandates or suffer some form of discrimination. We have recently passed through about 10,000 cases of COVID in the last six months. If that’s not evidence to say that the vaccines aren’t effective, then I don’t know what is. However, I’m not here tonight to talk about the ineffectiveness of the vaccine, which didn’t stop transmission.
I’m here to talk about how unsafe the vaccines are, and I want to explain why; I want to go through the biochemistry.
The COVID virus has 29 proteins in it. Normally, if you gave someone a deattenuated vaccine, you would take out the ionised molecule of that virus. So, if you’ve got 29 molecules, you’d take out one, and the one you’d take out is the ionised molecule. An ion either has more electrons than protons or, likewise, more protons than electrons. Either way, it’s a charge, and that’s what they call the active ingredient in a vaccine. If you’ve got two magnets, one with a north pole and one with a south pole, and the magnets go past each other, they want to attach. That’s why a vaccine is normally deattenuated. They take out that ionised molecule so it doesn’t go around jumping on everything. But what that does is it allows the antibody to attack the antigen, end of story.
The other thing is that, because that molecule is still quite large—with 28 molecules remaining in a normal deattenuated vaccine—it is too big to cross the endothelium. What is the endothelium? It is the small capillary between your muscle tissue and your bloodstream. In order to cross that capillary, you’ve got to be small enough, in a process called endocytosis, to cross into the bloodstream. What this particular vaccine does is it delivers a lipid nanoparticle. It is a very tiny particle, much smaller—by a factor of 1,000—than a normal virus. What that means is it can travel from the tissue, through the endothelium and into your bloodstream.
Now, we know that’s the way this particular vaccine works because if you go to table 4.2 in the TGA nonclinical evaluation report, you will see where they have done the distribution of the lipid nanoparticles on the lab rats—literally—when they injected this particular vaccine. I’ll read out some of the body organs that it went through and the concentration increases. For a start, I want to focus on the ovaries. The concentration levels are milligrams to each gram. By the end of the first 25 minutes, it was 0.1. By the end of the first day, it was 5.25. By the end of the second day, it was 12.26. That has doubled after two days.
And that’s not the only organ. It went into the liver, the heart, the eyes, the brain, the bone marrow, the bladder and the adrenal glands. Just about half of the vaccine’s lipid nanoparticles go into organs other than the injection site. This is despite the fact that we were told that a normal vaccine goes into your deltoid muscle and that’s where it stays. Well, that’s not the case with this particular vaccine.
And what’s particularly scary about this is that they knew this in the animal trials, and despite the fact that the concentration was still increasing after 48 hours, do you know what they did? They stopped the trial. Don’t you think you would run the trial right through to the point of where the lipid nanoparticles had left the body? They didn’t do that.
But that’s just the start of it, because once it gets inside the cell and starts creating the spike protein, that can last for days longer. But here’s the thing—in the animal trials they never delivered the spike protein mRNA inside the lipid. They delivered a benign enzyme by the name of luciferase, which is the stuff you see in fireflies, and that lights up so that they could trace it. But, as the TGA nonclinical report says, they never tested the distribution and degradation of the spike protein for this particular vaccine in any humans or animals before they rolled it out.
Normally, when you get the virus, it comes in through your mucosal system, and if the immunoglobulin A in your mucosal system doesn’t kill the virus it’ll eventually get into your systemic blood system. Your mucosal system is driven by immunoglobulin A; your systemic blood system is driven by immunoglobulin G. Once the virus gets in, in order to get inside the cell, it needs to rely on what they called the ACE receptor—which is the angiotensin-converting enzyme—and also the transmembrane serine protease, which is another enzyme. That has to carry the virus across your cell membrane, because your membrane is there to protect the organelles inside the cell—that is, your nucleus, your ribosome and your mitochondria in particular—from external forces. What this particular vaccine does is it makes the lipid catatonic. That means it uses transfection—it’s like when you’re cooking sausages on the barbecue and you see blobs of fat merge together. That’s exactly what happens with transfection. There is no barrier with this particular vaccine to the lipid going into any cell. Not only does it not stop at the deltoid but it also goes all throughout the body, and it can go into any cell because of the way they designed this lipid nanoparticle.
Once it’s inside the cell, normally—now this is a first. Normally, when you get the vaccine, you get the antigen and it doesn’t go anywhere near your cell. Once it goes into your cell, it goes into the part of your cell called the ribosome, which translates the mRNA. That ribosome will produce a protein. Normally, the spike protein on the virus is not the same as the spike protein in the vaccine. But, no, what they’ve done is replace the nucleotide uracil and put in a new nucleotide called methylpseudouridine. That was shown in studies, in 2005, to actually evade the immune system and have greater self-amplifying properties. In other words, it creates more proteins.
Not only did they modify the mRNA that way; they added another 70 adenine nucleotides at the end of the mRNA strand. Normally, there are about 30 adenine nucleotides at the start of the mRNA strand, but they’ve added another 70. What does that mean? It means the spike protein lasts a lot longer inside your cell, creating a toxic substance or a toxic molecule that is ionised in an unregulated manner. What I mean by an unregulated manner is that it relies on your immune system to kick in, come in, and destroy your cells. A normal vaccine doesn’t do any of that. It stays inside your deltoid muscle. It doesn’t go anywhere because it’s too big to travel.
So what we’ve got now is a vaccine that has delivered a protein in an unregulated manner. That’s similar to a pathway of cancer, where, basically, you get the unregulated reproduction of toxic molecules. Then it relies on your own body’s immune system to attack your cells. Where you have your body attacking your own cells, you’re now creating a pathway similar to acquired immune deficiency syndrome. If it goes wrong, you do not want your own body attacking your own cells.
The next step after that is, effectively, a concentration. When it comes through your mucosal system, if you have a strong, healthy immune system, the immunoglobulin A in that immune system should stop it from getting into your bloodstream. When it’s injected directly into your bloodstream, all you’re getting is an IgG response. You are not getting an IgA response. So when they said, early on, it was going to stop transmission, that was a blatant lie. And why was it? Anyone that understands anything about immunology knows that you need an immunoglobin A response to kill the actual virus in your mucosal system, because if you don’t kill it in the mucosal systemic you can still transmit it.
The paper did show that you got an immunoglobin G response, and that lasted for up to 35 days in monkeys. But those monkeys only weighed 10 kilograms and they were given three times the dose given to humans. It was a greater dose of about 20 times. You could argue that—35 divided by 20 days—maybe, the immunoglobin G response might have lasted for two days.
The other point is that, by doing it this way—the pathways they were using—they never tested this before they put it into humans. They never tested it for genotoxicity studies, despite the fact that this was the first time they ever put genes inside a body, and it’s synthesised genes. They never did longitudinal testing, they never did carcinogenic testing, and they never tested it for other drugs. So people who take other drugs, especially immunosuppressants—they never tested for that.
Well, that was Senator Gerard Renick, a representative for Queensland. Isn’t it disappointing that the Australian Senate was essentially empty there when Senator Renick was giving his speech? It reminded me of the UK Parliament in my country when Andrew Bridgen was giving his speech about various concerns related to health topics, and I think there were about seven MPs in the whole house. It’s almost as if our elected representatives are quite happy to hear some information but don’t want to hear other information. Of course, I couldn’t possibly comment, but I thought you’d like to hear those two speeches. Thank you for watching.
Posts tagged:

Site Notifications/Chat:
- Telegram Post Updates @JourneyToABetterLife (channel)
- Telegram Chatroom @JourneyBetterLifeCHAT (say hi / share info)
- Gettr Post Updates @chesaus (like fakebook)
Videos:
 Aussies
Aussies Or Buy me a Coffee (PayPal)

References

![[Rant] Satan-Claus Canada #WeWontForget](https://pennybutler.com/wp-content/uploads/2023/01/Canadian-Satan-Claus.jpg)